Starting a business is a big achievement for many entrepreneurs, but maintaining one is the larger challenge. There are many standard challenges that face every business whether they are large or small. It is not easy running a company, especially in a fast-paced, ever-changing business world. Technology advances, new hiring strategies, and now, political changes coming with the new administration, all add to the existing business challenges that entrepreneurs, business owners, and executives have to deal with.
Maximizing profits, minimizing expenses and finding talented staff to keep things moving seem to be top challenges for both SMBs and large corporations. We have been interviewing companies from around the world to discover what challenges they are facing in their businesses. We also asked each company to share business advice they would give to a younger version of themselves.
Below is our interview with Randal Haworth M.D., CEO at The Haworth Instiute:
What does your company do?
Though technically a company, I don’t consider us a company in the traditional sense. This is simply because I consider our clients not as consumers but as patients first and foremost. We do not sell them goods per se, our patients buy a specific medical service which I consider to be among the best aesthetic plastic surgery available. The Haworth Institute provides both surgical and nonsurgical aesthetic procedures employing the latest RF and laser technology for removal of both hair as well as wrinkles, skin tightening and appearance.
What is your role? What do you enjoy most about your role?
I am the surgical director of the Haworth Institute which is comprised of both my clinical practice in Beverly Hills as well as a surgical center and Self-Centered Aesthetics, my nonsurgical medi-spa, helmed by the very talented Katherine Braun RN. The most gratifying part of my work is what I call the circle of change. This circle starts when our team greets our patients from all walks of life around the globe and make them feel right at home. Needless to say, the technical aspects of plastic surgery are immensely satisfying. When I am able to meet their original aesthetic goals, the circle of change is complete and that is the best part of all.
What are the biggest challenges in your business right now?
Running a busy plastic surgical practice is very demanding to say the least. What is particularly challenging is to remain on point at all times. This involves not only creating beautiful results in the very competitive environment of Beverly Hills but also to screen out a sizable number of people seeking unrealistic results and those with problematic personality disorders. Believe me, in this day and age driven by media and litigation, hiring the wrong employee or operating on a patient wanting surgery for all the wrong reasons can be disastrous.
If you could go back in time, what business advice would you give to a younger version of yourself?
The number one thing with business is to have trusted my gut, especially before hiring employees. Obviously plastic surgery involves a lot more than that but running the business side of things is a different matter. Some people are better than that others and it does require discipline in order to bypass your cerebral side. As with any business, having a passion for your work is a must for success but it is not the only thing. It is akin to just looking at your feet when you walk. Having a clearly defined long-term goal is akin to also seeing the horizon-this requires disciplined work habits and structure which I wish I learned earlier on in my career.
Plastic surgeon Randal Haworth, MD, is taking the next step in his career with the launch of a stylish, comprehensive aesthetic care facility.
Randal Haworth, MD, made a name for himself in aesthetics in the early 2000s when he joined Fox television’s reality show, “The Swan.” On the program, he was part of a team of plastic surgeons, stylists and makeup artists who dramatically transformed participants’ appearances, Earlier this year, he transformed his own Beverly Hills, California-based practice when he moved to a new, custom-designed facility that incorporates a full range of aesthetic services—from facials and nutritional services to fillers, lasers and surgical procedures.
Dr. Haworth’s design philosophy for the new Haworth Institute was nature meets high-tech.
“It’s a beautiful place, and all our services are under one roof—the surgical center, my clinic and our new noninvasive center, Self Centered Aesthetics,” says Dr. Haworth. “Patients always asked us, ‘What else can you do?’ ‘How do I maintain this?’ It just doesn’t make sense nowadays not to offer the full-range of aesthetic treatments.”
In addition to laser treatments and injectables performed by Dr. Haworth and his R.N., celebrity esthetician John Tew performs signature facials and naturopathic doctor Matea Polisoto, who goes by “Dr. Matea,” offers IV therapy and nutrition counseling. “Like John, she has a very big following in Beverly Hills and beyond,” says Dr. Haworth. “She is involved with IV therapy, which helps augment the pre- and postoperative surgical experience, and optimizes healing.
“The people working with me are just as important as the surgeon—it’s all about having a team,” he says.
The Frustrated Artist
Born in Los Angeles and educated in England, Dr. Haworth has a somewhat unusual background for a Beverly Hills plastic surgeon. “My dad was English and spent World War Il in London selling bootleg whiskey during the Blitzkrieg. My mother and her family lived in Holland during the German occupation,” he says.
Following the war, both of his parents immigrated to the United States seeking opportunities, of which there were few in post-war Europe. “They met, and I was born in Los Angeles. But my dad always wanted me to be in England eventually,” says Dr. Haworth.
When he was 9 years old, he and his parents drove to Central America and boarded a cargo ship to England. During his school years in London, Dr. Haworth became enamored with the arts. “l always drew—and I was very good at a young age. In University I joined band. I was really into the arts, and that’s what I wanted to pursue,” he says. “But my parents, being war babies, wanted a doctor in the family and I was their only child.”
During a road trip prior to his final year at the university, he shared his goals with his parents. “We were in a VW bus and they said, ‘We’ll disown you if you become an artist. Make your decision’—it was really bizarre,” he says. His mind flashed back to a BBC interview of Kurt Wagner, MD, he had seen when he was 13. “l said, ‘Then I’ll be a plastic surgeon,’ having no idea what was involved in that.”
He came back to the U.S. and enrolled in medical school at the University of Southern California. Following graduation, he completed a five-year general surgery residency at Cornell Medical Center in New York. Dr. Haworth made his way back to the West coast for his plastic surgery residency at the University of California, Los Angeles.
“After my residency, I had no money so I was anxious to go into practice. I thought, well then I have to goto Beverly Hills because that’s where successful plastic surgeons go,” he says.
Another surgeon offered to rent him a space in his clinic’s kitchen, which was housed in one of the most desirable medical buildings in Beverly Hills. “He had a little pocket door in front of the kitchen so I stayed in there,” says Dr. Haworth. “During my clinic days, I would take his diplomas off the walls in the two little exam rooms and put mine up, and that’s how it started.
“l look back fondly on those days now, but it was horrible at the time. If I had two surgeries in a month, it was a great month.
Finding His Niche
During his UCLA residency, Dr. Haworth won a plastic surgery research prize for his lip surgeries, which provided a unique niche with which to build his practice, More than 20 years later, he has patients from all over the world who travel to the Haworth Institute for their lip surgeries.
“You can be the best doctor in the world, but if you don’t have marketing, no one will know about you,” he says. “So I leveraged that award and started getting known for lips, even though my favorite surgeries are noses, mid- facelifts and what I call hyperaesthetic surgeries where we change everything. The lips are what I was known for, and now I get jazzed by that because there’s really no competi- tion in the world for these surgeries.”
He offers upper, lower and corner lip lifting procedures as well fat transfer and F.A.T.M.A. (fat transfer & mucosal advancement). “l do many types of lip lifts because it is shape before volume; there are many things that fillers alone cannot do,” he says.
Embracing and Investigating New Technologies
Despite the limitations of traditional filling techniques, Dr. Haworth has embraced dermal fillers as effective tools to perfect his patients’ lips. In some cases the new, less invasive procedures are even surpassing what he can achieve in the O.R.
“Our mouths get wider as we age and our lower teeth become visible,” he says. “People will often just fill the lower lip horizontally, which won’t help with these concerns.”
In his surgical center, he performs lower lip V-Y plasty procedures to narrow the mouth, lift the bottom lip and pout out the middle third of the lower lip. But, due to the minimal improvement, he recently became interested in the idea of using vertical filler injections to lift and shape the lower lip.
“About three months ago, I started injecting vertically into the lower lip. I place my long cannula or a long needle vertically from the bottom of the prejowl sulcus all the way to where I see the needle blanching on the vermillion on the back of the lower lip on the sides. Then I inject vertically as I pull the needle out,” he says. “l am seeing such dramatic elevation of not just the lower lip but the whole corner of the mouth—the marionette folds are dramatically reduced and the labiomental sulcus opens up.”
He is calling this the Caisson technique after Caisson beams in construction. “The patients are three months out now, and the results are far better than what we see with the lower V-Y plasty in hiding the lower teeth,” he says.
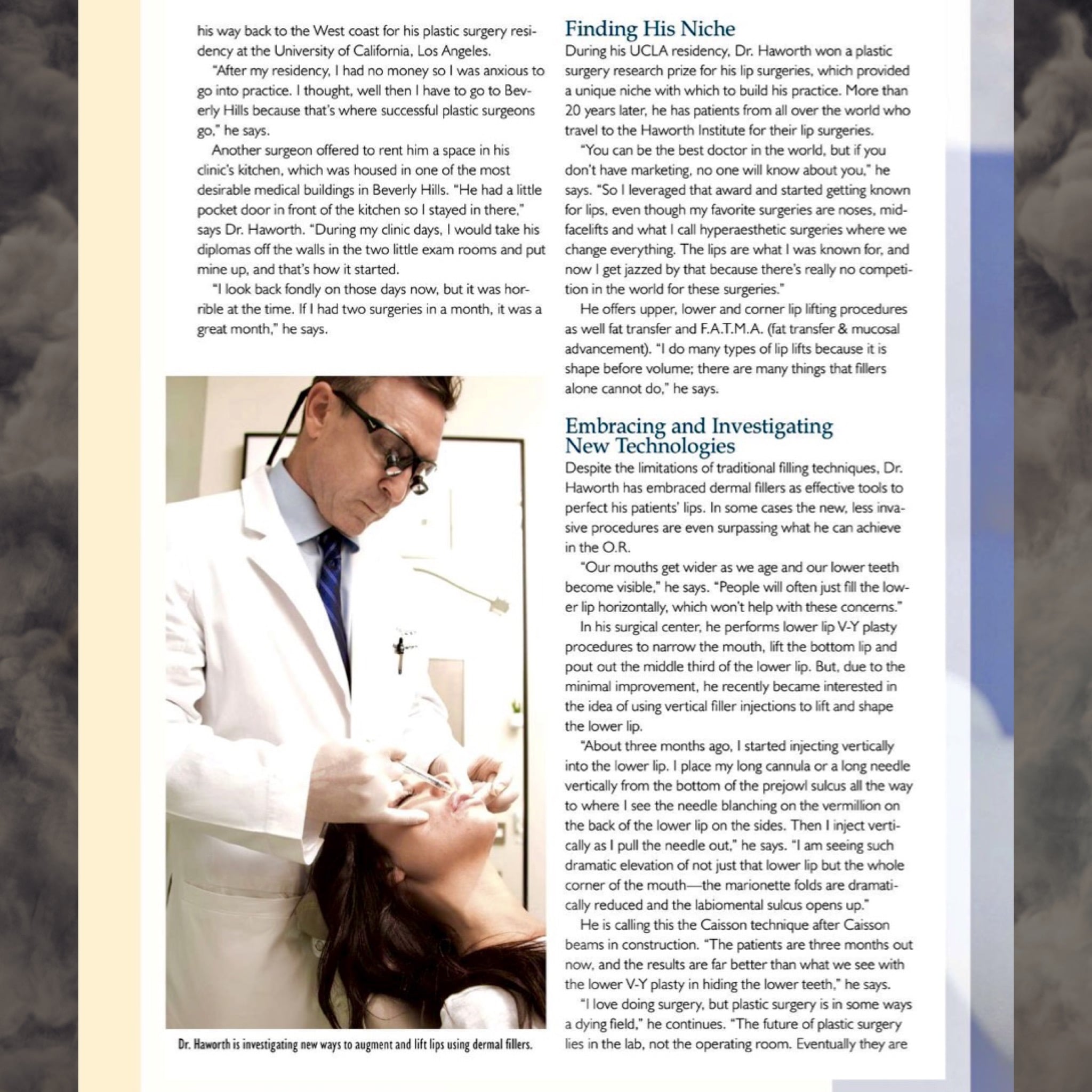
Dr. Haworth is investigating new ways to augment and lift lips using dermal fillers.
“l love doing surgery, but plastic surgery is in some ways a dying field,” he continues. “The future of plastic surgery lies in the lab, not the operating room. Eventually they are going to know how to stop senescence. In the meantime, the future of aesthetics is laying more and more in lasers and newer, better fillers, and I want to stay on the forefront of that.”
His biggest challenge is determining which new technologies and procedures live up to the hype—and resisting the urge to bring in every new device about which patients inquire. “Sixty to seventy percent of all new medical cosmetic technologies overpromise and under deliver,” he says. “First it’s a big ‘Wow!’ Then results are ‘operator-dependent,’ then it’s gathering dust, so I vet all these technologies and only offer the ones I believe are proven to work.
“What I want to offer my patients with the Haworth Institute and Self Centered Aesthetics is more than one-stop aesthetics, It’s the tools and knowledge to deliver the absolute best treatments for their individual concerns and lifestyles,” continues Dr. Haworth. “We have a turbocharged armamentarium of proven noninvasive treatments to carry on the philosophy that I espouse in my surgeries, which is really detailed aesthetic work.”
Beverly Hills-based plastic surgeon, Randal Haworth, M.D., says he needs to be comfortable and free to move in order to perform facial and body plastic surgery.
But space can be somewhat limited in an OR inside a boutique plastic surgery practice, he says.
“… so careful planning of the envisioned flow between patient, surgeon, scrub tech, circulating nurse and anesthesia provider must be done,” Dr. Haworth says. “In my case, I had to work with a rectangular operating room, in which case I first had to decide where the anesthesia machine would be situated, since its range of movement would be limited by the oxygen and vacuum hoses tethering it to the ceiling. Consequently, it was important for me to have a 180-degree turning radius for the operating table, so I could position it according to whether I am performing facial or body surgery. Of course, OR lights have to follow suit and must be very mobile and bright. My Trumpf LED [Trumpf Medical] system fits the bill nicely.”
2. A Quality Monitor and Sound System
Having a big monitor with a good sound system for music is not only a luxury but a necessity for the modern plastic surgeon. Having the monitor in constant view is a must, according to Dr. Haworth.
3. Intelligently Designed Cabinetry
Proper cabinetry, design to maximize space and efficiency, is essential, according to Dr. Haworth.
“You can never have too many cabinets from the get-go, since these promote organization and obviate the need for vulgar retrofits in the future,” he says. “When it comes to designing my clinic or the operating room, I think that creating and maximizing the feeling of unrestricted space is important for both the patient’s sense of security and the staffs’ sense of clarity.”
4. Don’t Cut Corners
Don’t cut expenses, when it comes to safety, according to Dr. Cohen.
5. Seek Expertise
Dr. Cohen says cosmetic surgeons should tap experts in designing operating rooms.
“Reach out to architects with experience in both the design and credentialing processes,” Dr. Cohen says. “Ultimately, certain third-party inspections may be required, and you don’t want to be caught off guard.”
Dos and Don’ts for the In-office OR
Erin Metelka, an interior designer with Studio Four Design, offers these design dos and don’ts.
OR Dos:
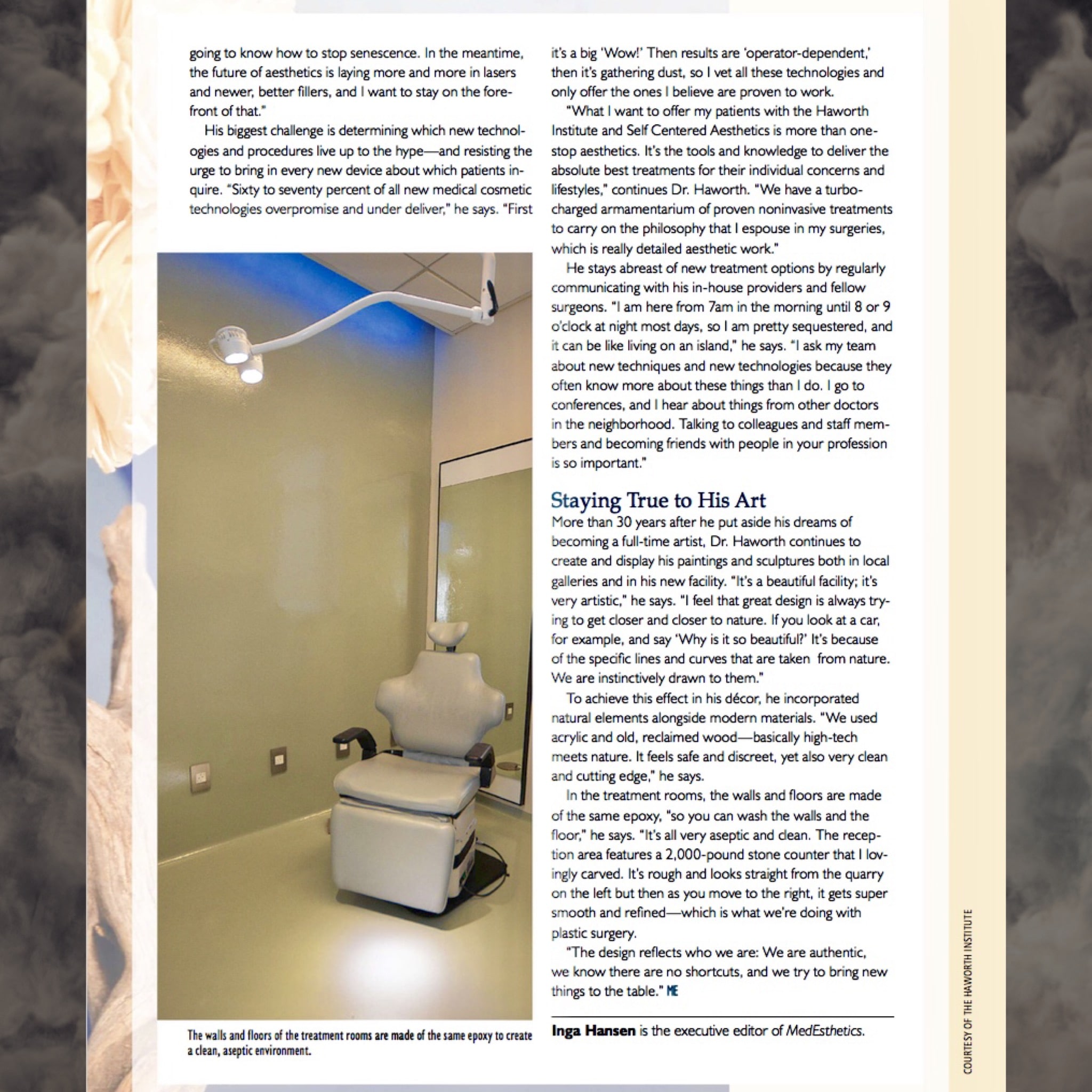
Use a sheet flooring, with heat welded seams and sanitary cove base.
Use bleach cleanable/non-porous products.
Use clean/calming colors.
Provide a variety of adjustable ambient lighting options.
Utilize floor patterns to designate the extents of the sterile zone and care-provider zones.
With the wide variety of procedures that occur in an operating room, often times, the table is moved in order to accommodate the most efficient workflow with the other equipment in the suite. The floor patterns can also be used to dimension the proper location of the table for these various scenarios.
When creating several operating rooms, utilize an identical layout (not mirrored). Often, physicians are moving into adjacent operating rooms for a procedure, while a room is being turned over and sterilized. Having identical layouts increases efficiency and reduces error.
OR Don’ts:
Do not have extraneous items of décor within the suite, such as artwork.
Do not utilize fabric of any kind such as curtains/draperies. If there are windows, create privacy with natural light by using integrated frosted glass. If an upholstery is required for a physician stool or other items, a bleach cleanable vinyl is a suitable alternative, ideally with a Crypton or nano-technology finish applied (these finishes work to prevent moisture penetration to the cushion and function as an antimicrobial).
Do not place any direct down-lighting, with the exception of the surgical boom, directly over the table.
As trifling as it may seem to the layperson, aesthetic surgery is serious business. Apart from obvious cosmetic ramifications, the seriousness becomes understandable when one considers that the surgeon must first make a healthy patient temporarily unwell in order to make he or she look better in the end. It is for this very reason plastic surgeons have an added unique responsibility which surgeons of other specialties simply do not bear. Choosing to undergo elective surgery is a series of decisions made by both the surgeon and the patient. As with all aspects of medicine, nothing is absolute, it is about controlling probability.
In this day and age, patients increasingly view plastic surgery as nothing more than a haircut with a short recovery, let alone one with a complication. Even under the best of hands, a complication can arise for any number of reasons and if it does, acting as a team with your surgeon is crucial. Whether following a facelift, rhinoplasty or any plastic surgery for that matter, almost all complications can be fixed in the end, even if multiple surgical revisions are needed.
It is normal for the layman to consider surgical results as either “good” or “bad”, but those adjectives can be misleading and are certainly inadequate in revealing the true story behind the result.
“Good” surgery with a complication is not the same as “bad” surgery per se. In other words, complications do not all come from “bad” surgeons and indeed, “bad” surgeons may have successfully completed an operation without encountering obvious complications. I think it fair to say most patients consider themselves as good people and if a complication happens to them, they will perceive themselves as victims of a bad surgery and by extension, a bad surgeon. So what is the difference between “bad” surgery and a “good” surgery with a complication?
Look at it this way… in any profession, there are the “good”, the “bad” and the “excellent”. For the sake of this discussion, let’s just oversimplify the comparison between “good” and the “bad”. Since plastic surgery is as much an art (or at least an artisanal craft) as it is a science, whereby results are measured both objectively and subjectively, it is not unreasonable to compare a plastic surgeon to any artist or craftsman, including sculptors, painters and woodworkers. Artists filter their talent and vision through years of experience to not only earn but continually solidify their reputation as either being “good” or “bad”. Moreover, good artists become respected by not just producing one “good” piece but doing so consistently, whereas the “bad” consistently create sub par results as judged by the median consensus.
However, all artists, whether good or bad, are limited by the quality of material with which they work. It is known that Michelangelo’s David has been deteriorating at a far more rapid pace than would be expected because of the poor quality of its marble composition. Bernini also broke a piece of marble in half through chiseling into an unexpected vein in the stone causing him to start all over with a brand-new block. Does that make him a bad artist? Hardly not.
In other words, complications happen and that’s why there are consents to protect not only the doctor but also the patient. Consents should ensure the patients are informed as to the shared risk both they and the surgeon take when undergoing surgery.
Many complications are avoidable. Both doctors and patients must do their part to optimize a certain outcome and minimize the risk of complications. Patients must avoid certain medications that may promote bleeding, cease all smoking for optimal circulation, follow instructions and take medications as prescribed. Otherwise, surgery may be self-sabotaged. On the other hand, surgeons must do their part in educating and performing the proper operation in the right patient with skill and dedication.
Other complications are unavoidable and just because they may be explainable in hindsight does not mean they were avoidable within the context they occurred. This is why it is paramount that patients disclose all of their medical history and follow their surgeon’s instructions to a T in order to minimize unexpected situations such as abnormal bleeding, poor wound healing, etc..
What spurred me to write this particular blog was a recent experience having performed a complex revision rhinoplasty on a dear friend of mine of 20 years. Unfortunately, this advanced detailed nasal reconstruction was exacerbated by unexpected physiological conditions including excessive bleeding and poor tissue characteristics. The next day, the patient presented with so much swelling underneath the pressure cast that it was being pushed off the face. The swelling was a hematoma which I immediately evacuated from under the skin (it was 4 1/2 mL, being the largest nasal hematoma encountered by either my colleagues or myself). Accompanying this was necrosis (death) of the columellar skin (the partition separating his left and right nostrils). This was particularly disappointing to say the least because the surgical results in terms of nasal shape, symmetry, tip definition and projection were otherwise excellent. Yet losing coverage over the columella would have serious ramifications.
Despite attempts to bring vascularized tissue using local intraoral flaps, my friend eventually needed the help of a certain specialist to bring fresh tissue to the columella below the nasal tip with a temporary forehead flap.
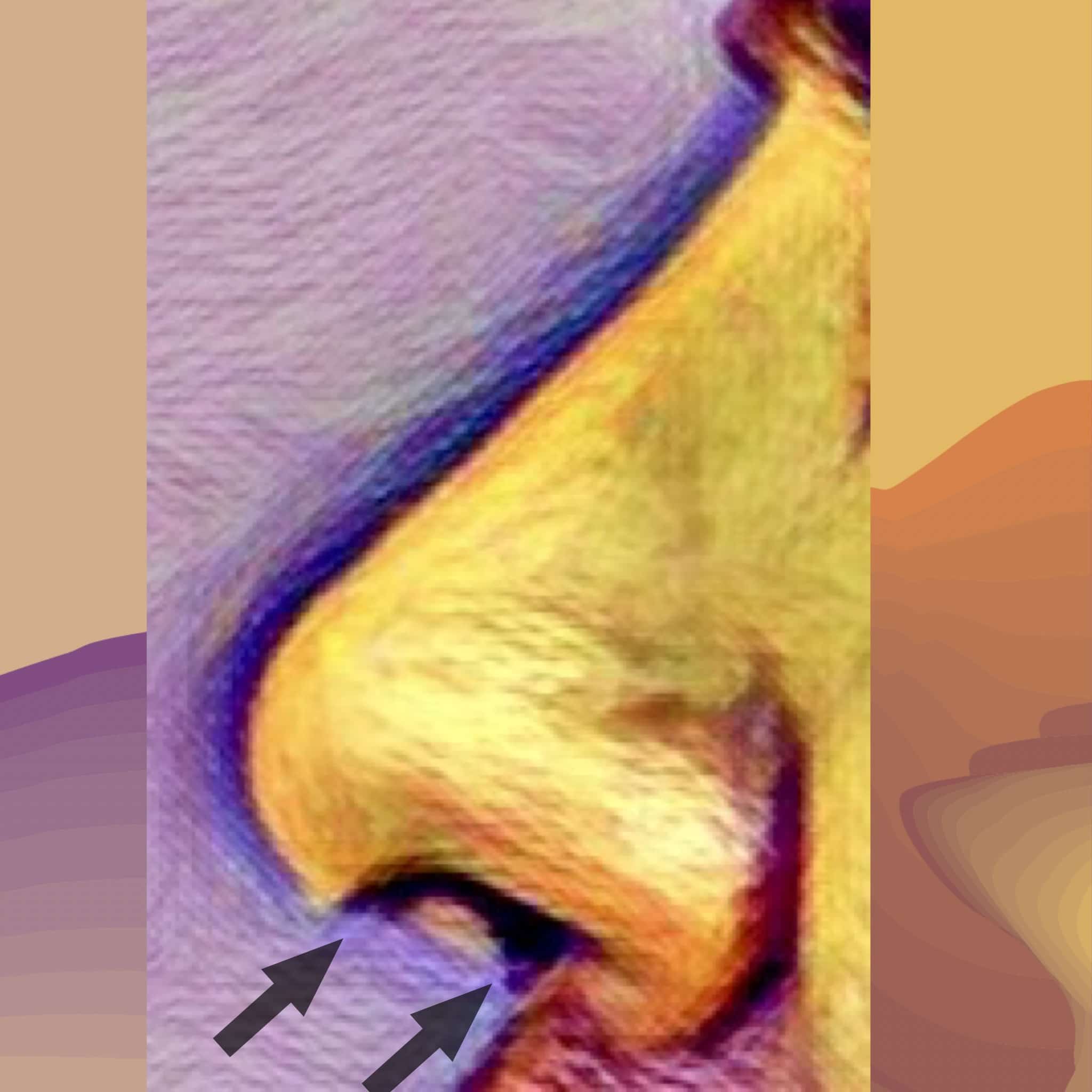
The arrows on the drawing illustrate that portion of the nasal skin (overlying the columella) that was necrotic. Replacement is required through vascularized tissue flaps
Albeit exceedingly rare, this 1.5 x 1.2 cm skin loss was enough to eradicate not only their trust in me as a surgeon but also our long term friendship. Most patients understandably experience a spectrum of emotions including panic, sadness, denial, anger and ultimately acceptance from a complication such as this. However, nothing could prepare me for the degree of ongoing vengeful anger and hostility the patient and their partner have directed towards me including threats to go to the press and ruin my reputation.
Anger is not only destructive but also lacks focus, therefore it can be especially counterproductive to both healing and a good result (not to mention friendship!). Premature castigations of blame fuel brash, illogical decisions which actually complicate the original complication.
Understanding the differences between “bad” and “good” surgery and “good” surgery with a complication can certainly help put things in perspective. When a patient concedes the net surgical aesthetic result, at least in terms of shape and symmetry, as good if not excellent, he or she is less likely to question, and more likely trust, their original choice of surgeon. Whether their breast lift incision opened or, as in this case, a small but strategic portion of nasal skin died, the affected patient will see the “bigger picture” and believe their surgeon will do the right thing by having their best interests at heart. This same patient understands that they were not necessarily a victim or unjustifiably punished by “bad” surgery. Instead, they will accept things for what they are, learn patience and develop a sense of optimism to set themselves up for the best possible outcome in the future.
The majority of complications concern wound healing and minor infections. For these, possible antibiotics and the “tincture of time” for healing to occur are required. Other times, simple, clinical interventions such as laser treatment, injections, the occasional scar revision and creams are all that are needed.
Other complications require more invasive solutions. Depending on the type of complication, an expeditious trip to the operatory maybe all that is required (e.g.,to drain a hematoma) whereas staged surgical revisions may be undertaken in the extremely rare case of tissue loss.
Most surgeons will recognize if a particular complication is beyond their level of expertise. A patient should not feel abandoned or simply passed off if they are referred to another expert if a complication warrants it. It is important to recognize that medicine is team work and the referral is simply a reflection of the original surgeon’s dedication to the best outcome possible.
Emotional advice after a complication
–Watch out for advice with an agenda. It is understandable that if a complication does arise, fear and anxiety will prompt you to seek solace and advice from friends and family members. While this is wholeheartedly encouraged, it is important to remember that not all the advice given is good especially considering that those giving advice are not often doctors nor do they know the intricate details of the patient’s particular case. Though most advice is well-meaning in intent, some may be motivated by guilt, jealousy, personality disorders or just plain ignorance. Furthermore, the advice a patient may obtain from elsewhere may be counterproductive because it may only increase their level of anxiety.
–Stay optimistic and avoid jumping to any pessimistic conclusions. It is not unheard of that acute anxiety will provoke a patient to impatiently reach for the help of an alternative plastic surgeon. Unfortunately, some plastic surgeons may be unscrupulous and advise the fragile, highly suggestible patient into unnecessary and ill-timed surgery claiming it is urgently needed to prevent some permanent deformity. Always keep a line of communication open with the original plastic surgeon to not only help allay personal fears but also be guided in the right direction with a second opinion if necessary.
After more than two decades of commitment to delivering the best of what plastic surgery can deliver in terms of aesthetic results and quality-of-life improvement, top Beverly Hills plastic surgeon, Randal Haworth, found it time to expand his philosophy into an adjacent arena. That arena is the nonsurgical approach to optimize the patient’s aesthetic wellness. Dr. Haworth has maintained that future advances in plastic surgery will not lie solely in the operatory but more in the laboratory. Specifically, advances in lasers, injectables, light and genomic therapy will take precedence over any evolutionary steps in surgical technique. Currently, non-surgical cosmetic procedures are rapidly evolving to meet the expectations, budgets and lifestyles of patients of all backgrounds and consequently, their popularity is exponentially increasing every year.
As a world-renowned expert in facial plastic surgery (including rhinoplasty, lip lifts, face lifts, eye lifts and even bodywork such as breast augmentation) Dr. Haworth has come to a point where he need not confine his artistry mainly to the syringe and scalpel but also safely and reliably imbue it into noninvasive aesthetic medicine. Consequently, he and his team at the Haworth Institute have founded Self-Centered Aesthetics, a center devoted to optimum physical appearance, through the safest, most reliable state-of-the-art technology.
Self-Centered Aesthetics (SLF-CA)will be catering to the vast majority of patients’ aesthetic needs.
Among the services SLF-CA will be offering are:
3. Removal of wrinkles, fine lines and sagging folds via a variety of methods including essentially all fillers, microneedling with PRP, Botox and lasers (Spectra®, Encore® Active and Deep FX™ fractionated CO2, ResurFX® fractionated erbium and IPL® Photofacial)
4. Treatment of brown spots, brown patches, red discolorations and spider veinsutilizing proven laser technology (IPL® Photofacial and Spectra®)
5. Tattoo removal(Spectra® and other lasers)
6. Noninvasive body fat reduction through SculpSure®, a laser designed to achieve up to 20% fat reduction in 25 minutes with virtually no discomfort and absolutely no incisions.
7. Facial feature improvementthrough the selective use of fillers and Botox®. With refined aesthetic sensibility and an astute artistic sensitivity, fillers (both temporary and permanent), can enhance all aspects of the face. However, to maximize the beauty of a result without artifice or outward fakery requires customized planning to balance patients’ needs with their individual expectations. From a flat forehead with hollow temples to sunken cheeks and dark eyelid circles to thin lips and an ill-defined jawline, the professionals at SLF-CA under the auspices of Dr. Haworth dedicate themselves to make you look your very best!
Additionally, our CENTER will offer aesthetician services to maintain and fine-tune your SELF and your AESTHETIC results.
Self-Centered Aesthetics™ will be coming soon. www.selfcenteredaesthetics.com
Well… as I originally predicted in a blog post at the time Kim Kardashian’s champagne-glass-bottom graced the cover of Paper magazine, there would be “fall out” to the story. Judging by active reaction to recent un-retouched photographs of Kim’s derrière in the media by both fellow plastic surgeons and public alike, comments have generally been less than flattering. Fortunate aftermath of wanton Buttock enlargement without consideration of body proportions and pulchritude
My blog post was essentially a warning to those seeking to “maxi-size” their assets in response to media’s insidiously pervasive influence on the public’s impressionable collective psyche.
A copy of my original blog post is here:I don’t like comic book butts and I cannot lie
Not to say that the images in question expose overtly ireversible droop of Kim’s buttocks, they do unquestionably reveal the dimpling, pitting and bulging of exaggerated cellulite. Furthermore, there is no way to predict how these artificially corpulent gluteals will age with further time. Unfortunately in 2017, there is little to be convincingly done to remedy such a situation.
Lest this be a caveat for those seeking buttock super-sizing regardless of the method employed.
Dr. Haworth
2017
I was exchanging breast implants and performing a capsulectomy the other day (to treat a breast encapsulation) when my anesthesia provider expressed surprise at my method. Specifically, she had commented that she has never worked with a breast implant revision specialist, especially one in Beverly Hills or California, who had removed the WHOLE collagenous capsule when treating a breast encapsulation. Apparently she has only seen plastic surgeons either make slits in capsules (capsulotomy) or only partially remove them.
Evidently, she was part of a growing support group of women who had their breast implants removed for mainly medical reasons and were firm believers that any associated capsules needed to be removed in their entirety during the same operation. Up to now I had no idea that performing a total capsulectomy is “a thing” and supposedly I am among a minority who do this par for the course.
One of the leading theories for breast encapsulation relates to bacteria and their byproduct, biofilm (a type of organic shield, if you will), surrounding the surface of the breast implant itself. One can safely assume that if a breast implant is supposedly contaminated by bacteria so is its associated surrounding capsule. Therefore, it is only logical to remove the collagen capsule in its entirety when removing or exchanging a breast implant, whether it be silicone or saline.
I created this video below to help patients better understand the vexing process of breast encapsulation and methods to treat it. Though breast augmentation is one of the most popular plastic surgical procedures performed today, it is also one of the most capricious or unpredictable because breasts often times have a mind of their own and do not behave in the way we would like them to.
Dr Haworth 2017
New techniques always emerge which supplant the old. The same is true with the plastic surgical procedure called rhinoplasty, or in common parlance, nose job. A nose is basically composed of three materials: overlying skin with associated fat, bone and cartilage.
A rhinoplasty involves:
changing the shape and slant of the bones through selective filing and cutting
changing the shape of the cartilages through removal, adding and reshaping with sutures and
in selected cases, “defatting” the skin to allow the shape of the cartilages and bone to “shine through”.
In order to perform the rhinoplasty, the surgeon must gain access to the underlying bone and cartilage through either through a closed or open technique. The former involves making incisions confined to within the nostrils and performing the surgery through the limited exposure that these incisions thus provide. The latter, open technique, involves making the same incisions within the nostrils but joining them across the columella (the fleshy partition that separates the left and right nostril at the base of the nose).
I am frankly surprised and amused that in 2017, some plastic surgeons still insist that the closed technique, when “performed properly”, provides equal or even superior results than those obtained with an open one. These same surgeons cite a few old masters of closed rhinoplasty fromthe 1970s and 80s to support their contention that the closed method is superior. However, the best results from these old Masters do not parallel those obtained from top rhinoplasty surgeons today. Whether you like it or not, progress is inevitable and the new masters of today produce better results than the masters of yore.
I recently attended two conferenceshosting some of the top thought leaders in rhinoplasty surgery. As expected, there was not one expert in the room who would consider closed rhinoplasty an option to achieve the delicate and precise results expected by their patients. Indeed, even in their hands they felt that a closed rhinoplasty generally leads to a subpar result. Imagine having to work on the engine of your car only through the left and right front wheel wells. Without opening the hood to gain full unimpeded access to the engine, your ability to effectively work is exceedingly hampered.
The results of any plastic surgery should be measured by the end visual result and not by the process to achieve it.
Those who promote closed rhinoplasty as better invariably cite less swelling and no potentially visible scar as their main selling point, but this is a fallacious argument. When properly performed, as a top Beverly Hills rhinoplasty expert, Dr Randal Haworth has seen minimal to no difference in postoperative swelling between the open and closed methods and the scars essentially become invisible whether you are a young model or a 70-year-old person. The proponents of closed rhinoplastyproudly display their early smooth and symmetrical resultsas being superior. However, in the early postoperative period, it is the very swelling that the closed proponents claim is not there that may be masking inaccurate nasal construction below. This can be seen in the many examples of famous nosesheralded in their early postoperative period but turn out poorly constructed when their swelling dissipated. Generally avoidable deformities such as inverted V deformities, pinched tips and crooked noses become unavoidably visible no matter how much makeup contouring and good lighting is available.
Famous Noses and Deformities via Closed Techniques:
After closed rhinoplasty with obvious ‘inverted V” deformity, pinched tip and lack of harmony between the upper and lower portion of the noseNote the lack of continuity between the upper bony portion of the nose and the lower cartilaginous portion. An obvious “inverted V” deformity and pinched tip do not help the situation.After a closed rhinoplasty, note crooked appearance, asymmetrical and drooping pinch tip
Examples of Complex Rhinoplasties Performed through the Open Technique:
Significant congenital asymmetry of the nostrils. After an open rhinoplasty-note significantly improved symmetry with minimal scar that a closed rhinoplasty technique can’t achieveUnfortunate result from a closed rhinoplasty with “inverted V” deformity and asymmetrical, bulbous tip. An open rhinoplasty was performed with significant improvement of the noseUnfortunate result from a closed rhinoplasty with “inverted V” deformity, retracted nostrils and asymmetrical, bulbous tip. An open rhinoplasty was performed with significant improvement of the noseUnfortunate result from a closed rhinoplasty with “inverted V” deformity, retracted nostrils and asymmetrical, bulbous tip. An open rhinoplasty was performed with significant improvement of the noseAnother example of noticeable congenital asymmetry of the nostrils. After an open rhinoplasty-note significantly improved symmetry with minimal scar that a closed rhinoplasty technique can’t achieve
When precise control over the shape and symmetry of the nose is required as well as control over the subtle light reflexes and shadows embodying the beauty of a nose, nothing beats an experienced surgeon with a precise touch, an aesthetic sensibility and an open rhinoplasty technique.
“Time is a cruel thief to rob us of our former selves. We lose as much to life as we do to death.” Elizabeth Forsythe Hailey
Living in the modern world becomes more complex and harder as life in the 21st-century becomes faster and faster. We are burdened with responsibilities and distracted by an interminable onslaught of media in all forms including the capricious internet. It seems as if everything is competing for our attention in one way, shape or form while stealing precious time we could otherwise devote to family, friends and simply to our own selves. Therefore, when it comes to saving time, the need to heal quickly after any cosmetic procedure is almost rapacious.
Unfortunately, there is no magic pill or formula to bypass the post operative inflammation of bruising, swelling and discomfort at this current time. As one of the top plastic surgeons in Beverly Hills, Dr. HAWORTH has seen a thing or two about how patients heal after the thousands of surgeries he has performed over two decades. As a facial plastic surgery expert, he has performed thousands of primary and revision rhinoplasties, brow lift, facelifts and blepharoplasties not to mention the breast implant operations throughout his career and has realized there are things you can do both at home and in the clinical setting to accelerate your healing.
First of all, it is a good idea to focus on whole foods as much as possible while avoiding processed ones as the former will contain the highest levels of vitamins and amino acids your body will need for a speedy recovery. Amino acids help wounds heal faster and obviously, these are found in chicken, meats, egg whites, fish, brown rice, healthy nuts like walnuts and almonds or sunflower seeds. Taking supplemental vitamin C in your diet while increasing zinc in your diet can be helpful. Instead of taking vitamin C for a bottle, you can eat strawberries, papayas and citrus fruits which are great sources of vitamin C. 500-1000mg is the usual amount that is taken. Zinc is found in oysters which have one of the highest levels of zinc found in any food. If you are going to take a supplement, 15 mg of zinc daily is the recommended amount but you can increase your zinc intake to 30–50 mg for 2 weeks before and 2 weeks after surgery, using zinc picolinate.
Beverly Hills plastic surgeon Dr. Haworth also recommends these useful supplements to take in preparation for your surgery include:
B12 and Iron – Iron and B12 both aid bone marrow in forming new blood cells, so incorporate foods like fish and eggs.
Vitamin B6250mg, twice a day for a week, starting 3 days after surgery. This helps reduce post-surgical fluid retention, such as swelling of the face, hands, feet or legs. With B6, you can experience substantial reduction within 24 to 48 hours.
CoQ10- Surgical trauma (particularly from cardiac surgery) causes an increase in free radicals, which damage cellular function. For this reason alone, you should take at least 50 mg of CoQ10 as part of your daily routine before your cosmetic surgery and 100–200 mg/day for at least 4 weeks after.
Fiber and probiotics – This combination helps boost the immune system and also keeps your digestive tract moving along. Eating yogurt with granola is just one easy way to get a serving of both fiber and probiotics! When choosing a probiotic, consider one that contains acidophilus and bifida bacteria (follow label instructions for dosage). Surgical patients often receive oral or intravenous antibiotics in the hospital, which creates the potential for yeast infections, digestive disturbances and diarrhea. A probiotic may help counteract these problems.
One amino acid that has been shown to speed with healing is glutamine and a study from Harvard and Dave showed that it shortened healing by about four days. Apart from supplements, glutamine can be found in beef, chicken and all types of fish. Dairy products such as cheese, milk, yogurt and eggs contain glutamine with ricotta and cottage cheese being the two richest sources. Vegetarians can find glutamine in beans and lentils.
For most of his patients, facial plastic surgery specialist Haworth recommends supplemental Arnica Montana, Bromelain/ Bromezyme (this pineapple enzyme helps prevent blood clots, aids digestion while decreasing inflammation and pain after surgery) and Pycnogenol/Pine bark. This triumvirate is aimed at reducing bruising, soreness and inflammatory edema.
Apart from the above, many patients inquire about any other additional medications, exercises or procedures that can be done to maximally reduce their healing times after surgery. Of course, all patients should ask their individual physicians or surgeons about their own personalized recommendations to speed up recovery which is beyond the scope of this post.
Bioptron® Light employs a combination of polarized infrared and visible light (480nm-3400nm) considered beneficial in the treatment of wound problems and injuries by exerting its effect at the cellular level. Bioptron® therapy has a low energy density (fluency) of 2.4 J/cm2 at a distance of 10 cm and can penetrate the skin up to 2.5 cm.
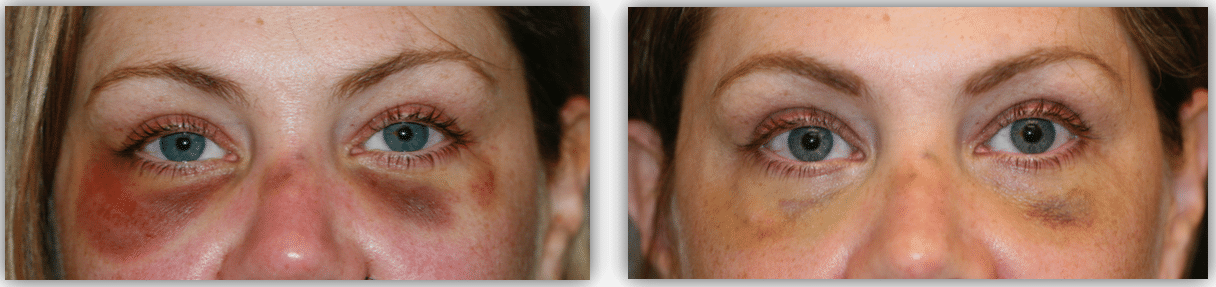
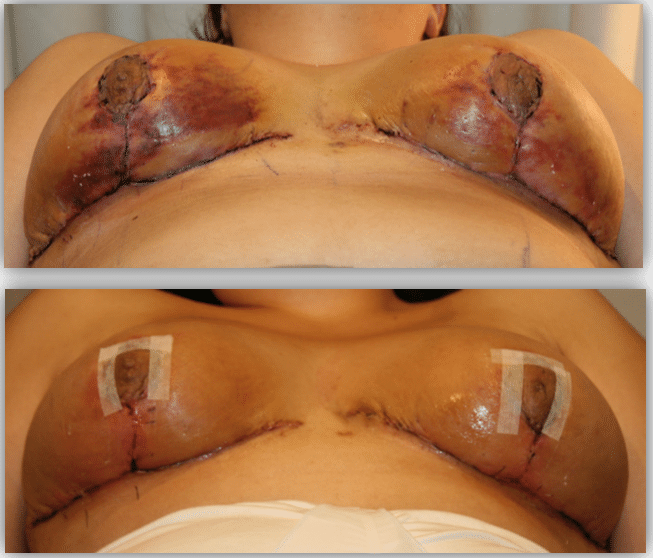
This patient had impending skin necrosis around her here after a facelift. Only 7 days of Bioptron ® light therapy were administered and notice the rapid improvement in reversing the damage.After 5 days of Bioptron® therapy to resolve bruising resulting from lower eyelid procedure to treat her dark circles/tear troughs.After 3 days of Bioptron® light therapy to accelerate the resolution of bruising and skin injury after a breast reduction by Dr. HAWORTH.
It has been used effectively in the treatment of burns, pressure sores, leg ulcers, wounds, pain and recently, postoperative healing. Dr Haworth have found it very useful in his clinic to reduce both swelling and bruising. Supporting his experience, other plastic surgeons here and abroad have noted decreased resolution times of eccymosis and edema following surgery by over 33% with Bioptron®. Indeed, it has been used to also reverse the course of cutaneous necrosis as well as accelerate granulation of open wounds, either alone or in conjunction with hyperbaric oxygen therapy (HBOT).
Hyperbaric oxygen therapy involves breathing pure oxygen in a pressurized room or tube. It is a well-established treatment for decompression sickness, a hazard of scuba diving. Other conditions treated with HBOT include serious infections, bubbles of air in blood vessels and non-healing wounds as a result of diabetes or radiation injury.
In a HBOT chamber, the air pressure is increased to 3 times higher than normal air pressure and under these conditions, your lungs can gather more oxygen than would be possible breathing pure oxygen at normal air pressure. However, there is some confusion about what actually is “true” HBOT. Those employing “soft” tent like enclosures are essentially useless since they are unable to obtain a true hyperbaric environment of 2 to 4 atmospheres absolute (ATA). In fact, these personal or home-use “hyperbaric” tent enclosures can usually only attain a pressure of 1.3 ATA. There is a debate as to how much and how many treatments are necessary to speed up recovery after plastic surgery. While most plastic surgeons perhaps recommend one preoperatively and at least 3 to 5 postoperatively, experts in the field say one needs at least 15 to 20 treatments in order to see significant results. In my experience, 3 to 5 treatments are all that is necessary to achieve the more modest goals of reducing edema, bruising and discomfort resulting from elective plastic surgery.
After certain surgeries, body contouring plastic surgery expert Dr Randal Haworth may also recommend selective lymphatic massage/drainage to resolve edema (swelling) of the extremities, particularly after liposuction or liposculpture.
The above aforementioned vitamins, nutritional supplements and clinical interventions may not be the panacea to surgical healing which comes in a pill form, but they certainly are a step in the right direction in making recovery from any procedure as smooth as possible in 2017.
Artificially round and hard appearing breasts after an overfilled “above the muscle” breast implant augmentation. The patient desired a more natural and smaller pair of breasts to match her frameNatural result afterexchange of her overfilled implants to memory gel silicone implants “under the muscle” along with a mastopexy (breast lift).
What is wrong with this revision breast implant and lift surgery I performed?
According to this patient, apparently everything!
At first, this patient came to me with ostensibly straightforward requests to “make” her breasts smaller and “better-shaped” in accordance with her body frame. Of note, she had undergone a previous “above the muscle” breast augmentation which, in my humble opinion, left her with a net result of breasts which were too big, too round and too fake. In essence, her breasts did not lend to a pulchritudinous appearance and that is why she sought my expertise in the first place. Indeed, she wanted to get remarried after having children and was seeking “christian boobs” to attract a decent husband. So I did what any self-respecting, honest and aesthetically minded board certified plastic surgeon would do and that was to perform a capsulectomy (remove her collagenous scar capsules), substitute her overfilled saline implants with smooth Memory Silicone Gel implants placed “under the muscle” and conclude with a bilateral mastopexy (breast lift). I thought the surgery was an unqualified success and, further punctuated by her exceptional healing vis-à-vis scarring.
So why was she unhappy? I was thoroughly puzzled since we both had extensive discussions prior to the surgery about the usual risks, alternatives and benefits including what she exactly wanted from the surgery. I know she wanted to go smaller (check), she wanted to be natural (check), she wanted to appear more youthful and perky (check) and indeed she conceded that I did achieve these goals. However,she also expected her breasts to be firm and more round –she felt that her result was too natural, both in look and to touch and therefore something went wrong.
BEFORE: Artificially round and hard appearing breasts after an overfilled “above the muscle” breast implant augmentation. The patient desired a more natural and smaller pair of breasts to match her frameAFTER:Natural result after exchange of her overfilled implants to memory gel silicone implants “under the muscle” along with a mastopexy (breast lift).BEFOREAFTER
But after further, protracted postoperative conversations with her, I realized where the disconnect was. I did not give her what she exactly wanted from the surgery because I gave her what she askedfor and not what she wanted. In essence, this was a story of missed and unrealistic expectations.
More and more of these situations arise in a plastic surgery practice simply because unrealistic expectations are instilled in us 24/7 by social media. The main platforms culpable for this insidious brainwashing are the mobile apps Instagram, Snapchat and YouTube with their interminable repository of Photoshopped/FaceTuned manipulated models and instructional contouring videos. Young women come to me wanting cheekbones, buttocks or breasts like Abigail or Jocelyn Instastar simply because they are famous and therefore more popular and loved.
Social media and Instagram star Abigail Ratchford
Indeed, one patient requested Bella Hadid’s nose even though, in my opinion her rhinoplasty ended up with an “inverted V” deformity and a somewhat pinched, boxy tip. However, it did not matter to her because she considered Bella her idol andwas willing to accept a possible substandard result with potential nasal obstruction. Ah, the power of celebrity!
Recently, I had the experience of operating on another young woman who had beautifully shaped breasts with a natural cleavage. She wanted to go only slightly bigger yet have a bigger gap between her breasts. The surgery went flawlessly but the patient was dissatisfied. She agreed her breasts were fuller with a wider cleavage but she now voiced that I should have known all along she wanted her breasts to look fake, round and hard! After this perplexing conversation, I sat down and pondered the meaning of what I really do.
Social media and Instagram star, Joselyn Cano.
It is one thing to make abnormalities such as unnatural breasts look natural but it’s another thing altogether to make natural looking breasts look deliberately unnatural and possibly unappealing. For decades, I have endeavored to create natural results by making the deformed normal and the normal beautiful but now a new aesthetic standard has emerged in our culture and ultimately, it may not have positive consequences.
But who am I to judge? Fake is the new real.
Randal Haworth MD, FACS