Many social media influencers enlist the help of photo editing apps to sharpen up their picture-perfect public image. Beverly Hills plastic surgeon Dr. Randal Haworth believes that Tammy Hembrow may also rely on cosmetic procedures. According to Dr. Haworth, she may have undergone a nose job, liposuction and dermal fillers to achieve her bombshell look. ‘Miss Hembrow is the quintessential Instagram model for our social media world where fake is the new real,’ Dr. Haworth said.
The celebrity plastic surgeon went on to claim that she strikingly different in recent photos compared to images of her taken several years ago. ‘Based on what I presume to be filtered photos, she has undergone a striking transformation of not only her facial features but also of her facial shape,’ Dr. Haworth claimed. ‘Her jawline is more defined into a “V-line”. I would even venture to say her chin has been shortened and narrowed compared to her teenage years.’ says Dr. Haworth.
According to Dr. Haworth, Tammy Hembrow’s lips have also almost certainly been enhanced due to their ‘overly plumped’ appearance. He claimed: ‘Like Kylie Jenner, Tammy has been originally inspired by the Angelina Jolie lip variety. Paradoxically, lips oversized for a face can mature the visage beyond its years.’ His claims come after Tammy was stretchered out of Kylie Jenner’s 21st birthday party at celebrity hotspot Delilah in West Hollywood last Thursday night.
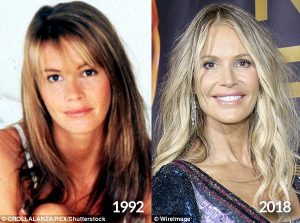
Elle Macpherson, has been an advocate of natural beauty, crediting an active lifestyle and a plant-based diet as the secrets behind her age-defying appearance. Beverly Hills plastic surgeon Dr Randal Haworth, believes that Elle may have also undergone a few cosmetic procedures to maintain her effortless beauty over the years. Dr Haworth stated: ‘The plan is simple when maintaining the beauty of an already beautiful woman. Elle’s genetic blueprint is flawless, therefore a plastic surgeon would have to follow the plan to a “T”, never veering away from her natural features.’
Dr Haworth believes that Elle may have had a subtle rhinoplasty in her thirties, resulting in ‘a squared nasal tip flanked by vertical grooves extending down to her nostril rims’. Dr Haworth also claims that she may have gone under the needle to enhance her already-striking visage. ‘Her lips are fuller in a subtle way, indicating she may have had them plumped with an off-the-shelf filler such as Juvéderm,’ he claimed. ‘These are some of the type of subtle “tweaks” that may have helped help Elle Macpherson radiate her natural beauty in a casual yet confident manner,’ he surmised.
Elle has made no secret of her laissez-faire approach to beauty and aging, telling This Morning in June that she is proud of her natural look. In 2016, Elle admitted PEOPLE magazine that she had played around with cosmetic procedures to fight wrinkles.
Rebecca Judd, is known for her glamorous and striking appearance. The Melbourne socialite has always denied plastic surgery rumors, a Beverly Hills plastic surgeon claims her flawless visage is far from natural. Dr. Randal Haworth said before and after photos suggest the Postcards presenter may have had ‘cosmetic fillers’ or a ‘fat transfer’ at some point.
‘Earlier, her eyes were deep set because they were surrounded by noticeable hollowing,’ Dr. Haworth said referring to photos of Bec from more than 10 years ago. ‘My most age-defying patients who make looking beautiful as effortless as breathing are the ones who work at it the hardest.’ Daily Mail Australia has reached out to Bec for comment. In 2013, the mother-of-four acknowledged that she invests ‘a lot of time, effort and cash’ into her appearance and said she gets ‘shocking eye bags.’ She previously credited Melbourne skin clinic Liberty Belle for her glowing skin and gets everything from exfoliation to laser treatments. In 2008, Bec, who is the wife of former AFL star Chris, denied plastic surgery rumours.
Megan Gale, has long been an advocate for aging gracefully, speaking openly about her views on plastic surgery and why she has chosen not to go under the knife. Beverly Hills plastic surgeon Dr. Randal Haworth has weighed in on Megan’s age-defying appearance. ‘I understand Megan has denied “going under the knife” and, based solely on her photographs, I tend to believe her,’ Dr. Haworth told Daily Mail Australia this week.
Dr. Haworth, who has not treated Megan himself, described several small, non-surgical procedures she may have undergone to maintain her supermodel look. Haworth also believes that Megan may have had some Botox ‘here and there’ to subtly smooth out her crow’s feet. Megan has spoken candidly about her attitudes toward cosmetic work in the past. In 2016 she told New Idea in 2016 that she would never consider surgery as her former AFL star partner Shaun Hampson, 30, would ‘kill her’.
Megan, who previously dated radio personality Andy Lee, is one of Australia’s most successful fashion exports. Throughout her career, she has graced the covers of countless magazines, including Marie Claire, InStyle, and GQ Australia.
Plastic surgeon Randal Haworth, MD, is taking the next step in his career with the launch of a stylish, comprehensive aesthetic care facility.
Randal Haworth, MD, made a name for himself in aesthetics in the early 2000s when he joined Fox television’s reality show, “The Swan.” On the program, he was part of a team of plastic surgeons, stylists and makeup artists who dramatically transformed participants’ appearances, Earlier this year, he transformed his own Beverly Hills, California-based practice when he moved to a new, custom-designed facility that incorporates a full range of aesthetic services—from facials and nutritional services to fillers, lasers and surgical procedures.
Dr. Haworth’s design philosophy for the new Haworth Institute was nature meets high-tech.
“It’s a beautiful place, and all our services are under one roof—the surgical center, my clinic and our new noninvasive center, Self Centered Aesthetics,” says Dr. Haworth. “Patients always asked us, ‘What else can you do?’ ‘How do I maintain this?’ It just doesn’t make sense nowadays not to offer the full-range of aesthetic treatments.”
In addition to laser treatments and injectables performed by Dr. Haworth and his R.N., celebrity esthetician John Tew performs signature facials and naturopathic doctor Matea Polisoto, who goes by “Dr. Matea,” offers IV therapy and nutrition counseling. “Like John, she has a very big following in Beverly Hills and beyond,” says Dr. Haworth. “She is involved with IV therapy, which helps augment the pre- and postoperative surgical experience, and optimizes healing.
“The people working with me are just as important as the surgeon—it’s all about having a team,” he says.
The Frustrated Artist
Born in Los Angeles and educated in England, Dr. Haworth has a somewhat unusual background for a Beverly Hills plastic surgeon. “My dad was English and spent World War Il in London selling bootleg whiskey during the Blitzkrieg. My mother and her family lived in Holland during the German occupation,” he says.
Following the war, both of his parents immigrated to the United States seeking opportunities, of which there were few in post-war Europe. “They met, and I was born in Los Angeles. But my dad always wanted me to be in England eventually,” says Dr. Haworth.
When he was 9 years old, he and his parents drove to Central America and boarded a cargo ship to England. During his school years in London, Dr. Haworth became enamored with the arts. “l always drew—and I was very good at a young age. In University I joined band. I was really into the arts, and that’s what I wanted to pursue,” he says. “But my parents, being war babies, wanted a doctor in the family and I was their only child.”
During a road trip prior to his final year at the university, he shared his goals with his parents. “We were in a VW bus and they said, ‘We’ll disown you if you become an artist. Make your decision’—it was really bizarre,” he says. His mind flashed back to a BBC interview of Kurt Wagner, MD, he had seen when he was 13. “l said, ‘Then I’ll be a plastic surgeon,’ having no idea what was involved in that.”
He came back to the U.S. and enrolled in medical school at the University of Southern California. Following graduation, he completed a five-year general surgery residency at Cornell Medical Center in New York. Dr. Haworth made his way back to the West coast for his plastic surgery residency at the University of California, Los Angeles.
“After my residency, I had no money so I was anxious to go into practice. I thought, well then I have to goto Beverly Hills because that’s where successful plastic surgeons go,” he says.
Another surgeon offered to rent him a space in his clinic’s kitchen, which was housed in one of the most desirable medical buildings in Beverly Hills. “He had a little pocket door in front of the kitchen so I stayed in there,” says Dr. Haworth. “During my clinic days, I would take his diplomas off the walls in the two little exam rooms and put mine up, and that’s how it started.
“l look back fondly on those days now, but it was horrible at the time. If I had two surgeries in a month, it was a great month.
Finding His Niche
During his UCLA residency, Dr. Haworth won a plastic surgery research prize for his lip surgeries, which provided a unique niche with which to build his practice, More than 20 years later, he has patients from all over the world who travel to the Haworth Institute for their lip surgeries.
“You can be the best doctor in the world, but if you don’t have marketing, no one will know about you,” he says. “So I leveraged that award and started getting known for lips, even though my favorite surgeries are noses, mid- facelifts and what I call hyperaesthetic surgeries where we change everything. The lips are what I was known for, and now I get jazzed by that because there’s really no competi- tion in the world for these surgeries.”
He offers upper, lower and corner lip lifting procedures as well fat transfer and F.A.T.M.A. (fat transfer & mucosal advancement). “l do many types of lip lifts because it is shape before volume; there are many things that fillers alone cannot do,” he says.
Embracing and Investigating New Technologies
Despite the limitations of traditional filling techniques, Dr. Haworth has embraced dermal fillers as effective tools to perfect his patients’ lips. In some cases the new, less invasive procedures are even surpassing what he can achieve in the O.R.
“Our mouths get wider as we age and our lower teeth become visible,” he says. “People will often just fill the lower lip horizontally, which won’t help with these concerns.”
In his surgical center, he performs lower lip V-Y plasty procedures to narrow the mouth, lift the bottom lip and pout out the middle third of the lower lip. But, due to the minimal improvement, he recently became interested in the idea of using vertical filler injections to lift and shape the lower lip.
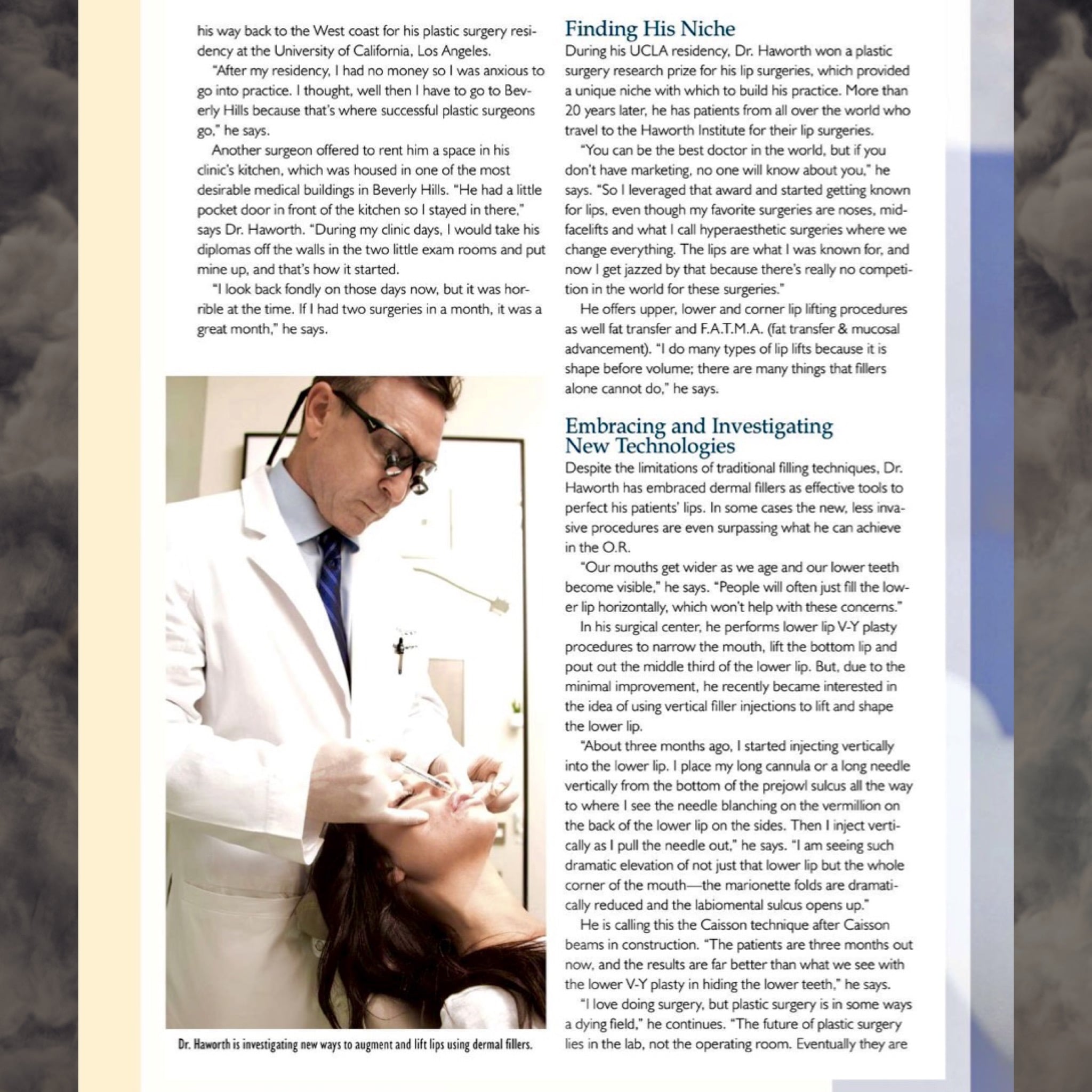
“About three months ago, I started injecting vertically into the lower lip. I place my long cannula or a long needle vertically from the bottom of the prejowl sulcus all the way to where I see the needle blanching on the vermillion on the back of the lower lip on the sides. Then I inject vertically as I pull the needle out,” he says. “l am seeing such dramatic elevation of not just the lower lip but the whole corner of the mouth—the marionette folds are dramatically reduced and the labiomental sulcus opens up.”
He is calling this the Caisson technique after Caisson beams in construction. “The patients are three months out now, and the results are far better than what we see with the lower V-Y plasty in hiding the lower teeth,” he says.
Dr. Haworth is investigating new ways to augment and lift lips using dermal fillers.
“l love doing surgery, but plastic surgery is in some ways a dying field,” he continues. “The future of plastic surgery lies in the lab, not the operating room. Eventually they are going to know how to stop senescence. In the meantime, the future of aesthetics is laying more and more in lasers and newer, better fillers, and I want to stay on the forefront of that.”
His biggest challenge is determining which new technologies and procedures live up to the hype—and resisting the urge to bring in every new device about which patients inquire. “Sixty to seventy percent of all new medical cosmetic technologies overpromise and under deliver,” he says. “First it’s a big ‘Wow!’ Then results are ‘operator-dependent,’ then it’s gathering dust, so I vet all these technologies and only offer the ones I believe are proven to work.
“What I want to offer my patients with the Haworth Institute and Self Centered Aesthetics is more than one-stop aesthetics, It’s the tools and knowledge to deliver the absolute best treatments for their individual concerns and lifestyles,” continues Dr. Haworth. “We have a turbocharged armamentarium of proven noninvasive treatments to carry on the philosophy that I espouse in my surgeries, which is really detailed aesthetic work.”
Recently, I was honored to be featured on the cover of the highly popular regarded trade magazine of the noninvasive aesthetic industry, MedEsthetics.
Here is the article. We at Self-Centered Aesthetics ™are super excited to be off to such a great, auspicious start. We are aiming to deliver the best, state of the art noninvasive treatment to all patients, under one roof with my philosophy of beauty.
Embracing Artistry
By Inga Hansen Photography by Cory Sorensen
Plastic surgeon Randal Haworth, MD, is taking the next step in his career with the launch of a stylish, comprehensive aesthetic care facility.
Randal Haworth, MD, made a name for himself in aesthetics in the early 2000s when he joined Fox television’s reality show, “The Swan.” On the program, he was part of a team of plastic surgeons, stylists and makeup artists who dramatically transformed participants’ appearances, Earlier this year, he transformed his own Beverly Hills, California-based practice when he moved to a new, custom-designed facility that incorporates a full range of aesthetic services—from facials and nutritional services to fillers, lasers and surgical procedures.
Dr. Haworth’s design philosophy for the new Haworth Institute was nature meets high-tech.
“It’s a beautiful place, and all our services are under one roof—the surgical center, my clinic and our new noninvasive center, Self Centered Aesthetics,” says Dr. Haworth. “Patients always asked us, ‘What else can you do?’ ‘How do I maintain this?’ It just doesn’t make sense nowadays not to offer the full-range of aesthetic treatments.”
In addition to laser treatments and injectables performed by Dr. Haworth and his R.N., celebrity esthetician John Tew performs signature facials and naturopathic doctor Matea Polisoto, who goes by “Dr. Matea,” offers IV therapy and nutrition counseling. “Like John, she has a very big following in Beverly Hills and beyond,” says Dr. Haworth. “She is involved with IV therapy, which helps augment the pre- and postoperative surgical experience, and optimizes healing.
“The people working with me are just as important as the surgeon—it’s all about having a team,” he says.
The Frustrated Artist
Born in Los Angeles and educated in England, Dr. Haworth has a somewhat unusual background for a Beverly Hills plastic surgeon. “My dad was English and spent World War Il in London selling bootleg whiskey during the Blitzkrieg. My mother and her family lived in Holland during the German occupation,” he says.
Following the war, both of his parents immigrated to the United States seeking opportunities, of which there were few in post-war Europe. “They met, and I was born in Los Angeles. But my dad always wanted me to be in England eventually,” says Dr. Haworth.
When he was 9 years old, he and his parents drove to Central America and boarded a cargo ship to England. During his school years in London, Dr. Haworth became enamored with the arts. “l always drew—and I was very good at a young age. In University I joined band. I was really into the arts, and that’s what I wanted to pursue,” he says. “But my parents, being war babies, wanted a doctor in the family and I was their only child.”
During a road trip prior to his final year at the university, he shared his goals with his parents. “We were in a VW bus and they said, ‘We’ll disown you if you become an artist. Make your decision’—it was really bizarre,” he says. His mind flashed back to a BBC interview of Kurt Wagner, MD, he had seen when he was 13. “l said, ‘Then I’ll be a plastic surgeon,’ having no idea what was involved in that.”
He came back to the U.S. and enrolled in medical school at the University of Southern California. Following graduation, he completed a five-year general surgery residency at Cornell Medical Center in New York. Dr. Haworth made his way back to the West coast for his plastic surgery residency at the University of California, Los Angeles.
“After my residency, I had no money so I was anxious to go into practice. I thought, well then I have to goto Beverly Hills because that’s where successful plastic surgeons go,” he says.
Another surgeon offered to rent him a space in his clinic’s kitchen, which was housed in one of the most desirable medical buildings in Beverly Hills. “He had a little pocket door in front of the kitchen so I stayed in there,” says Dr. Haworth. “During my clinic days, I would take his diplomas off the walls in the two little exam rooms and put mine up, and that’s how it started.
“l look back fondly on those days now, but it was horrible at the time. If I had two surgeries in a month, it was a
great month,” he says.
Finding His Niche
During his UCLA residency, Dr. Haworth won a plastic surgery research prize for his lip surgeries, which provided a unique niche with which to build his practice, More than 20 years later, he has patients from all over the world who travel to the Haworth Institute for their lip surgeries.
“You can be the best doctor in the world, but if you don’t have marketing, no one will know about you,” he says. “So I leveraged that award and started getting known for lips, even though my favorite surgeries are noses, mid- facelifts and what I call hyperaesthetic surgeries where we change everything. The lips are what I was known for, and now I get jazzed by that because there’s really no competi- tion in the world for these surgeries.”
He offers upper, lower and corner lip lifting procedures as well fat transfer and F.A.T.M.A. (fat transfer & mucosal advancement). “l do many types of lip lifts because it is shape before volume; there are many things that fillers alone cannot do,” he says.
Embracing and Investigating New TechnologiesDespite the limitations of traditional filling techniques, Dr. Haworth has embraced dermal fillers as effective tools to perfect his patients’ lips. In some cases the new, less invasive procedures are even surpassing what he can achieve in the O.R.”Our mouths get wider as we age and our lower teeth become visible,” he says. “People will often just fill the lower lip horizontally, which won’t help with these concerns.”In his surgical center, he performs lower lip V-Y plasty procedures to narrow the mouth, lift the bottom lip and pout out the middle third of the lower lip. But, due to the minimal improvement, he recently became interested in the idea of using vertical filler injections to lift and shape the lower lip.”About three months ago, I started injecting vertically into the lower lip. I place my long cannula or a long needle vertically from the bottom of the prejowl sulcus all the way to where I see the needle blanching on the vermillion on the back of the lower lip on the sides. Then I inject vertically as I pull the needle out,” he says. “l am seeing such dramatic elevation of not just the lower lip but the whole corner of the mouth—the marionette folds are dramatically reduced and the labiomental sulcus opens up.”He is calling this the Caisson technique after Caisson beams in construction. “The patients are three months out now, and the results are far better than what we see with the lower V-Y plasty in hiding the lower teeth,” he says.Dr. Haworth is investigating new ways to augment and lift lips using dermal fillers.”l love doing surgery, but plastic surgery is in some ways a dying field,” he continues. “The future of plastic surgery lies in the lab, not the operating room. Eventually they are going to know how to stop senescence. In the meantime, the future of aesthetics is laying more and more in lasers and newer, better fillers, and I want to stay on the forefront of that.”His biggest challenge is determining which new technologies and procedures live up to the hype—and resisting the urge to bring in every new device about which patients inquire. “Sixty to seventy percent of all new medical cosmetic technologies overpromise and under deliver,” he says. “First, it’s a big ‘Wow!’ Then results are ‘operator-dependent,’ then it’s gathering dust, so I vet all these technologies and only offer the ones I believe are proven to work.”What I want to offer my patients with the Haworth Institute and Self Centered Aesthetics is more than one-stop aesthetics, It’s the tools and knowledge to deliver the absolute best treatments for their individual concerns and lifestyles,” continues Dr. Haworth. “We have a turbocharged armamentarium of proven noninvasive treatments to carry on the philosophy that I espouse in my surgeries, which is really detailed aesthetic work.”
What is Beverly Hills Plastic Surgeon, Dr Randal Haworth’s, latest tool to minimize bruising with injections?
Injection techniques to place filler into the face to correct lines, folds and wrinkles have became even more advanced with the use of blunt tip cannulae, such as Dermasculpt.
These are similar to needles except that they are not sharp and therefore are less prone to cut the tiny diameter blood vessels in and below the skin.
What does this mean for the patient?
-Markedly less bruising
-Generally significant less discomfort
-Greater safety profile
I don’t employ them to treat all areas of the face, since certain anatomical facial features require extremely precise placement of filler not afforded by blunt tip cannulae. They are ideal to inject larger areas which require generalized plumping or filling such as the temples, cheek hollows, brows and jawline.
I have injected most types of filler through them including Juvederm, Restylane, Belotero, Artefill, Aquamid and Radiesse.
Be prepared to hear some minor crackling noise, however, for the first minute or so similar to lettuce being cut!
Botox may soon be used to treat psychological depression. We know that it can help alleviate the symptoms of migraines in many.
Dr. Randal Haworth Beverly Hills is an expert specialist in facial plastic surgery including maintenance therapy through fillers and paralytic agents such as Botox®, Dysport® and Xeomen®.
Botulinum toxin A seems to do far more than just block the transmission of acetylcholine (the neurotransmitter chemical released from nerve endings to affect change in muscle, glands etc.).
There is new evidence to suggest that Botulinum toxin type A can be used to treat depression which was first reported in 2006 by two American doctors (Finzi E, Wasserman E “treatment of depression with botulinum toxin A: a case series, Dermatol Surg 2006; 32 (five): 645-649). Based on this small study, a much larger study with careful patient assessment has shown that a single treatment of the glabellar lines (the dreaded “11” frown lines) with botulinum toxin resulted in a significant and sustained benefit for depressed patients (Wollmer MA, de Boer C, Kalak N, et al. “facing depression with botulinum toxin: a randomized controlled trial,” Journal of psychiatric research May 2012; 46 (five): 574-581).
Therefore, one can conclude that Botox®, through control of facial expression, seems to have the ability to control patient mood. However, is this an effect of increased self-confidence on the patient’s part or is this a result of hormone or regulatory peptide secretion as well?
Who knows at this time, but this is intriguing nonetheless. Dr. Haworth of Beverly Hills, however, is still not offering this treatment for depression even though many do say that aesthetic plastic surgery can be surgical psychiatry when performed in properly selected patients! Is this why there are so many ostensibly happy people in Beverly Hills and and its environs? 😉
Over the last 3 to 4 years I, as a primary and revision rhinoplasty specialist, have noticed an increasing and disturbing trend being practiced amongst those facial and classic plastic surgeons in my immediate community of Beverly Hills and other cities. This trend revolves around the use of rib grafts for not only revision but also primary rhinoplasty (!) (or in common parlance, nose job).
A good number of rhinoplasties require cartilage in order to achieve exemplary results. Cartilage is used to either build a bridge, fill depressions, augment or support the nasal tip. It is mainly harvested from the septum (that partition that exists in the midline of the nose which separates the left and right nostril) or the ear. Though I am fully trained general surgeon and am comfortable operating in and around the lungs and heart, I rarely employ rid graft as a source of cartilage. For most, it is generally a last resort when absolutely no other cartilage source is available. Admittedly, rib provides a strong support and is generally in plentiful supply. However, a number of downsides arise when rib is harvested: a permanent visible scar is created below the breast. Additionally, significant pain can arise from the harvesting as well as a small chance of creating a pneumothorax (or a collapsed lung) . Finally, rib can be notorious for warping thereby creating a nose that is crooked.
Despite these drawbacks, I will use rib when there is a collapsed nasal septum (or dorsum creating a saddle nose deformity) or when plentiful cartilage is needed while other sources are exhausted.
See the accompanying photos.
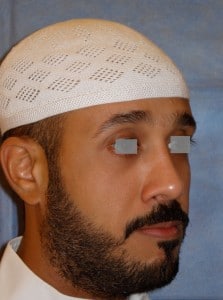
A Collapsed Nasal Bridge or Saddle-Nose Deformity
After a Revision Rhinoplasty Utilizing Rib Graft
A Severe Saddle-nose Deformity after Infection
After Rib Graft Reconstruction
I always use cartilage to highlight and augment the nasal tip, however, when there is not enough cartilage present and I only need to build the bridge by a small amount, I do not hesitate to employ some artificial material such as Goretex®. I utilize this only when the chance of infection is remote. When patients are properly selected for utilizing Goretex®, the chance of infection extremely minimal in my experience. Unfortunately, the surgeons who habitually use rib grafts will scare the bejesus out of their patients into choosing the rib graft method by overstating the chance of infection and poor outcome if Goretex® is used.
So if I am writing that rib grafts are over utilized, then why do the rib graft cartel tell their patients otherwise?
I feel it is simply a matter of finance. When a rib graft is harvested, the surgeon can charge a lot more for both his services and the operating room, especially if insurance is billed. Most patients will not question their surgeon’s motivated choices and indeed, feel that they have no choice at all, believing that the rib-graft-mafia method is their only solution.
What is especially unsettling is that these doctors who are members of the rib graft cartel are now utilizing rib grafts for primary rhinoplasties (first time nose jobs). This is very puzzling because there is plenty of prime cartilage graft material available from the septum and ear and there is little to no reason to subject the patient to a rib surgery.
All I can say is that this is a dangerous trend which introduces unnecessary risk and morbidity to the operation.
A good patient is an educated patient and the purpose of my blog is to merely propagate information in the most objective way possible so that patients can make their own decisions as sentient adults. To learn more about primary and revision rhinoplasty , you can click here.
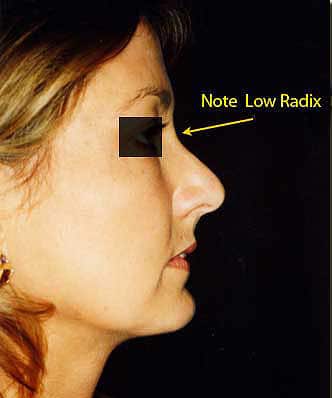
This lesser known anatomic point of the nose is often purposely overlooked by rhinoplasty specialist surgeons because of the challenges it poses to those attempting to alter it. It is represented by the angle formed by the uppermost portion of the nose as it blends into the forehead proper. Yes, altering this area does have a subtle, yet profound influence upon the final appearance of a nose job- it can differentiate an excellent result from a “so-so” one. The surgeon can raise the radix so that the nose blends into the forehead at a higher latitude as well as softly elevate the natural valley that can exist at this are if it is too deep. Furthermore, one can deepen the radix if too much bone is present between the eyeball and the bridge on profile view.
The ideal position of the radix lies approximately at the latitude of the upper eyelash/upper eyelid crease. Beverly Hills plastic surgeon, Dr Randal Haworth can raise it by placing a precisely shaped softened cartilage graft (usually harvested from the nasal septum or ear) with beveled edges onto the bone of the radix area. Alternatively the radix or nasion can be rasped or chiseled with specialized delicate instruments to a lower, deeper position.
Why does raising a radix from a low position improve the final appearance of a nose? Well, imagine two noses which are identical in shape and forward projection except that one has a low radix while the other has a high one. The one with the low radix is shorter compared to the one with the high. Now imagine two men, both with the same 34 inch waist, but one is short while the other tall. Who appears fatter? The short person does, of course. This same optical illusion applies to the nose with a low radix-it appears as it projects further out from the face as compared with the one with the higher radix and not necessarily in an attractive way.
The following photos represent a beautiful result of a corner lip lift and concomitant rhinoplasty in which the radix was raised.
Note where her radix point lies. It is lower than the level of her eyelash, making the nose look more projecting than it really is.
The result after a corner lip lift and a rhinoplasty with Radix enhancement.
Work here results in some extra swelling localized to the space between the eyebrows in the sense that it lasts a few days longer. Dr Haworth at the Haworth Institute has a few tricks up his sleeve to accelerate the resolution of the nasal swelling by injecting a dilute mix of Kenalog under the skin (and it is relatively painless) two weeks out. This “turbocharges” the swelling to go away!
Of course, the radix can also be augmented with a filler of some sort, such as fat, Radiesse, Juvederm, Aquamid and Artefill.

 According to Dr. Haworth, Tammy Hembrow’s lips have also almost certainly been enhanced due to their ‘overly plumped’ appearance. He claimed: ‘Like Kylie Jenner, Tammy has been originally inspired by the Angelina Jolie lip variety. Paradoxically, lips oversized for a face can mature the visage beyond its years.’ His claims come after Tammy was stretchered out of Kylie Jenner’s 21st birthday party at celebrity hotspot Delilah in West Hollywood last Thursday night.
According to Dr. Haworth, Tammy Hembrow’s lips have also almost certainly been enhanced due to their ‘overly plumped’ appearance. He claimed: ‘Like Kylie Jenner, Tammy has been originally inspired by the Angelina Jolie lip variety. Paradoxically, lips oversized for a face can mature the visage beyond its years.’ His claims come after Tammy was stretchered out of Kylie Jenner’s 21st birthday party at celebrity hotspot Delilah in West Hollywood last Thursday night.
 Dr Haworth believes that Elle may have had a subtle rhinoplasty in her thirties, resulting in ‘a squared nasal tip flanked by vertical grooves extending down to her nostril rims’. Dr Haworth also claims that she may have gone under the needle to enhance her already-striking visage. ‘Her lips are fuller in a subtle way, indicating she may have had them plumped with an off-the-shelf filler such as Juvéderm,’ he claimed. ‘These are some of the type of subtle “tweaks” that may have helped help Elle Macpherson radiate her natural beauty in a casual yet confident manner,’ he surmised.
Dr Haworth believes that Elle may have had a subtle rhinoplasty in her thirties, resulting in ‘a squared nasal tip flanked by vertical grooves extending down to her nostril rims’. Dr Haworth also claims that she may have gone under the needle to enhance her already-striking visage. ‘Her lips are fuller in a subtle way, indicating she may have had them plumped with an off-the-shelf filler such as Juvéderm,’ he claimed. ‘These are some of the type of subtle “tweaks” that may have helped help Elle Macpherson radiate her natural beauty in a casual yet confident manner,’ he surmised.

 Megan Gale, has long been an advocate for aging gracefully, speaking openly about her views on plastic surgery and why she has chosen not to go under the knife. Beverly Hills plastic surgeon Dr. Randal Haworth has weighed in on Megan’s age-defying appearance. ‘I understand Megan has denied “going under the knife” and, based solely on her photographs, I tend to believe her,’ Dr. Haworth told Daily Mail Australia this week.
Megan Gale, has long been an advocate for aging gracefully, speaking openly about her views on plastic surgery and why she has chosen not to go under the knife. Beverly Hills plastic surgeon Dr. Randal Haworth has weighed in on Megan’s age-defying appearance. ‘I understand Megan has denied “going under the knife” and, based solely on her photographs, I tend to believe her,’ Dr. Haworth told Daily Mail Australia this week.