
Botox may soon be used to treat psychological depression. We know that it can help alleviate the symptoms of migraines in many.
Dr. Randal Haworth Beverly Hills is an expert specialist in facial plastic surgery including maintenance therapy through fillers and paralytic agents such as Botox®, Dysport® and Xeomen®.
Botulinum toxin A seems to do far more than just block the transmission of acetylcholine (the neurotransmitter chemical released from nerve endings to affect change in muscle, glands etc.).
There is new evidence to suggest that Botulinum toxin type A can be used to treat depression which was first reported in 2006 by two American doctors (Finzi E, Wasserman E “treatment of depression with botulinum toxin A: a case series, Dermatol Surg 2006; 32 (five): 645-649). Based on this small study, a much larger study with careful patient assessment has shown that a single treatment of the glabellar lines (the dreaded “11” frown lines) with botulinum toxin resulted in a significant and sustained benefit for depressed patients (Wollmer MA, de Boer C, Kalak N, et al. “facing depression with botulinum toxin: a randomized controlled trial,” Journal of psychiatric research May 2012; 46 (five): 574-581).
Therefore, one can conclude that Botox®, through control of facial expression, seems to have the ability to control patient mood. However, is this an effect of increased self-confidence on the patient’s part or is this a result of hormone or regulatory peptide secretion as well?
Who knows at this time, but this is intriguing nonetheless. Dr. Haworth of Beverly Hills, however, is still not offering this treatment for depression even though many do say that aesthetic plastic surgery can be surgical psychiatry when performed in properly selected patients! Is this why there are so many ostensibly happy people in Beverly Hills and and its environs? 😉
For further information click on this link to body language.net
Tag: Dr Randal Haworth
The Perfect Lower Eyelid-No Wrinkles, No Hollow Circles
What is the perfect lower eyelid?
We all want to have the eyelids when we were 20 with minimal-to-no wrinkles, no bags, no dark circles and a smooth transition from the lower eyelid into a nice full elevated cheekbone.
But life tends to throw us a curveball. As we get wiser, our wrinkles get proportionately deeper.
80% of this is hardwired into our genetics while 20% is in our hands. In other words, genetics is our gun and the environment is our trigger.
The best treatment is prevention by avoiding environmental toxins-tobacco smoke, harsh chemicals and sun exposure are the three main culprits that come to mind.
The second treatment is maintenance through the use of hygiene, moisturizers and strategic use of topical antioxidant therapy. Among the latter is a dizzying and bewildering array of botanicals, herbals, vitamins, roots, vegetables, nutritional supplements and berries! But the two most singularly effective treatments are the use of vitamin A (derivatives of retinol, Retin-A, etc.) and fat-soluble vitamin C. The early use of these substances goes a long way in helping to prevent and diminish the wrinkles in the first place. I know many 60+ year old patients who have virtually no crows feet (without the use of Botox™) because they have been using a derivative of Retin-A for close to 20 years.
The third and final treatment is direct physical intervention through the use of either lasers, Botox™/Xeomen™, fillers (Restylane®, Juvederm®, etc) and/or plastic surgery. Plastic surgery on the lower eyelid is called blepharoplasty and can consist of any combination of skin removal, fat bag reduction and eradicating the dark circles/hollows that frame the lower eyelid from the cheek.
As a Beverly Hills plastic surgeon dealing with the most discerning of patients, I perform lower eyelid rejuvenation every day in my practice. Any blepharoplasty specialist is well aware of the potential pitfalls of performing surgery on the lower eyelid. The most dreaded complication that patients are fearful of is a changed lower eyelid shape (that “pulled down” look that was so frequent in surgery before the 1990s).
In the vast majority of cases I do remove skin through what I call a lower lid pinch technique utilizing one single stitch. This minimizes any chance of lower eyelid retraction. This scar basically heals as an invisible one, one which needs a magnifying glass to visualize. Though I still reduce protruding fat bags on occasion, the frequency with which I do perform this has dropped precipitously in the last 10 years. In the majority of cases, transferring fat with extreme sensitivity and appreciation of the delicate eyelid anatomy, will not only significantly diminish the dark circles but also hide any protruding fat pockets around the lower eyelid.
Fat transfer, if properly performed, is by-and-large permanent around the lower eyelid and should be performed by extremely experienced plastic surgeons. While adhering to this principle, the incidence of lower eyelid irregularity and small bumps can be vastly diminished.
Contact The Haworth Institute for further information.
We all want to have the eyelids when we were 20 with minimal-to-no wrinkles, no bags, no dark circles and a smooth transition from the lower eyelid into a nice full elevated cheekbone.
But life tends to throw us a curveball. As we get wiser, our wrinkles get proportionately deeper.
80% of this is hardwired into our genetics while 20% is in our hands. In other words, genetics is our gun and the environment is our trigger.
The best treatment is prevention by avoiding environmental toxins-tobacco smoke, harsh chemicals and sun exposure are the three main culprits that come to mind.
The second treatment is maintenance through the use of hygiene, moisturizers and strategic use of topical antioxidant therapy. Among the latter is a dizzying and bewildering array of botanicals, herbals, vitamins, roots, vegetables, nutritional supplements and berries! But the two most singularly effective treatments are the use of vitamin A (derivatives of retinol, Retin-A, etc.) and fat-soluble vitamin C. The early use of these substances goes a long way in helping to prevent and diminish the wrinkles in the first place. I know many 60+ year old patients who have virtually no crows feet (without the use of Botox™) because they have been using a derivative of Retin-A for close to 20 years.
The third and final treatment is direct physical intervention through the use of either lasers, Botox™/Xeomen™, fillers (Restylane®, Juvederm®, etc) and/or plastic surgery. Plastic surgery on the lower eyelid is called blepharoplasty and can consist of any combination of skin removal, fat bag reduction and eradicating the dark circles/hollows that frame the lower eyelid from the cheek.
As a Beverly Hills plastic surgeon dealing with the most discerning of patients, I perform lower eyelid rejuvenation every day in my practice. Any blepharoplasty specialist is well aware of the potential pitfalls of performing surgery on the lower eyelid. The most dreaded complication that patients are fearful of is a changed lower eyelid shape (that “pulled down” look that was so frequent in surgery before the 1990s).
In the vast majority of cases I do remove skin through what I call a lower lid pinch technique utilizing one single stitch. This minimizes any chance of lower eyelid retraction. This scar basically heals as an invisible one, one which needs a magnifying glass to visualize. Though I still reduce protruding fat bags on occasion, the frequency with which I do perform this has dropped precipitously in the last 10 years. In the majority of cases, transferring fat with extreme sensitivity and appreciation of the delicate eyelid anatomy, will not only significantly diminish the dark circles but also hide any protruding fat pockets around the lower eyelid.
Fat transfer, if properly performed, is by-and-large permanent around the lower eyelid and should be performed by extremely experienced plastic surgeons. While adhering to this principle, the incidence of lower eyelid irregularity and small bumps can be vastly diminished.
 |
 |
|
| Wall, aging lower eyelid showing crepey lower eyelid skin, bags and mild hollowing | After a lower blepharoplasty (eyelid tuck) removing excess skin, excess protruding fat bags and performing strategic fat transfer into the lower eyelid circles (hollows) | |
 |
 |
|
| This patient has the classic signs of lower eyelid aging including excess eyelid skin with wrinkles, protruding fat bag and mild hollowing (dark circles) | After lower blepharoplasty (eyelid tuck) performed by Dr. Randal Haworth of Beverly Hills. In the surgery, he removed excess eyelid skin, reduce the excess bags of fat and performed judicious fat transfer in the dark circles |
Contact The Haworth Institute for further information.
Bad Posture = Droopy Breast Augmentation
As being one of the leading breast augmentation and implant revision specialists in Beverly Hills, Dr. Randal Haworth has noted how important a part posture plays in enhancing the breast appearance. Women with rounded shoulders impart a bigger, heavier look to their breasts, almost matronly if you will. By squaring off the shoulders, not only does a silicone or saline breast augmentation look more perky and youthful, but also a heightened feminine self-confidence is implied.
Certainly not a “slacker” look 😉
For further information, go to http://www.drhaworth.com/breast-augmentation/
Follow Dr Haworth on Twitter: @drhaworth
 |
 |
|
| How rounded shoulders associated with bad posture can change breast augmentation results | Note How Good posture Enhances the Breast Augmentation Result |
Open vs Closed Rhinoplasty in Beverly Hills
In order to perform a nose job or rhinoplasty whether in Beverly Hills, Los Angeles or wherever, the plastic surgeon must be physically able to manipulate only two things under the nasal skin-cartilages and bone, Well, the debate rages on and on as to what is the best of the two methods in gaining access to the internal cartilaginous and bony structures of the nose. The two methods are the “closed” and “open” techniques.
The “closed” technique involves creating incisions confined solely to within the actual nose (usually located just within the nostrils proper) whereas the “open” utilizes the same incisions as the “closed” but also incorporates a small additional one across the columella (the fleshy partition separating the left and right nostril at the bottom of the nose).
In this age of less invasive surgery afforded by modern technology through the use of endoscopes, modern radiology, etc. one would think that the “closed” technique represents a newer evolution in rhinoplasty surgery, but surprisingly, the opposite is true. The “closed” technique is the more traditional approach while the “open” evolved and gained in popularity as both patient and surgeons expectations grew. Perhaps unrealistically, patients increasingly expect perfection and in their quest to deliver the acme of results, surgeons need as much control as possible when performing the surgery. Control involves extremely accurate symmetrical suture placement (to reshape cartilage), hemostasis (to minimize bleeding), strategic cartilage graft location and stabilization among other factors. In order to gain the most control as possible, visibility must be maximized and this is where the “open” method far surpasses the”closed”.
Proponents of the “closed” technique cite prolonged swelling and a potentially visible scar across the columella as two distinct disadvantages to the “open”. However, in proper hands these supposed shortcomings can almost always be avoided. I, as a rhinoplasty specialist, used to perform 80% of my rhinoplasties as “closed”, but now I carry out 90% as “open” and I can safely say that over 95% of my rhinoplasty patients are delighted with their new nose by the end of the second week. If the surgery is carefully undertaken, I have seen essentially no difference in swelling between the “closed” and “open” techniques. However, the one difference I have seen are the clearly superior results afforded by the “open” method.
To see many “open” rhinoplasty results, click here and here for revision rhinoplasty.
Dr Randal Haworth can be contacted at 310 273 3000 and Is a Board Certified Plastic Surgeon (American Board of Plastic Surgery) who practices at The Haworth Institute in Beverly Hills.
The “closed” technique involves creating incisions confined solely to within the actual nose (usually located just within the nostrils proper) whereas the “open” utilizes the same incisions as the “closed” but also incorporates a small additional one across the columella (the fleshy partition separating the left and right nostril at the bottom of the nose).
In this age of less invasive surgery afforded by modern technology through the use of endoscopes, modern radiology, etc. one would think that the “closed” technique represents a newer evolution in rhinoplasty surgery, but surprisingly, the opposite is true. The “closed” technique is the more traditional approach while the “open” evolved and gained in popularity as both patient and surgeons expectations grew. Perhaps unrealistically, patients increasingly expect perfection and in their quest to deliver the acme of results, surgeons need as much control as possible when performing the surgery. Control involves extremely accurate symmetrical suture placement (to reshape cartilage), hemostasis (to minimize bleeding), strategic cartilage graft location and stabilization among other factors. In order to gain the most control as possible, visibility must be maximized and this is where the “open” method far surpasses the”closed”.
Proponents of the “closed” technique cite prolonged swelling and a potentially visible scar across the columella as two distinct disadvantages to the “open”. However, in proper hands these supposed shortcomings can almost always be avoided. I, as a rhinoplasty specialist, used to perform 80% of my rhinoplasties as “closed”, but now I carry out 90% as “open” and I can safely say that over 95% of my rhinoplasty patients are delighted with their new nose by the end of the second week. If the surgery is carefully undertaken, I have seen essentially no difference in swelling between the “closed” and “open” techniques. However, the one difference I have seen are the clearly superior results afforded by the “open” method.
To see many “open” rhinoplasty results, click here and here for revision rhinoplasty.
Dr Randal Haworth can be contacted at 310 273 3000 and Is a Board Certified Plastic Surgeon (American Board of Plastic Surgery) who practices at The Haworth Institute in Beverly Hills.
The Bulbous Nasal Tip In Rhinoplasty
Dr. Haworth of Beverly Hills gained much of his advanced experience as both a primary and revision rhinoplasty specialist back in the Middle East. He performed literally hundreds of nose jobs there on patients from all walks of life. One of the most common complaints there are boxy and bulbous nasal tips.
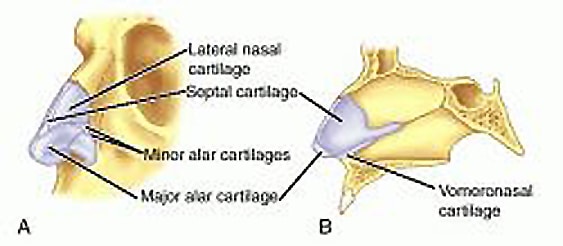
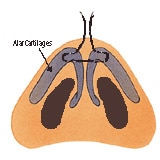
What constitutes a bulbous nasal tip?The bulbous nasal tip is most likely caused by thick alar cartilages (see accompanying diagram)and/or alar cartilages that are splayed out instead of shaped in a neat triangular formation. |
||||||||||||||
 |
||||||||||||||
This anatomic situation can be exacerbated by a thick layer of oily, sebaceous nasal tip skin. Think of the latter as a sleeping bag as opposed to a thin silk sheet., draped over delicate structures
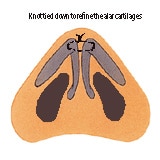
How does an experienced plastic surgeon correct the thick bulbous nasal tip during a nose job?In my hands, I prefer performing a rhinoplasty utilizing an “open” approach because it affords me vital binocular vision so I can assess up to half-a-millimeter asymmetries that otherwise I would would be unable to appreciate utilizing a closed approach. The closed approach is one where the incisions are solely confined to the inner rims of the nostril, whereas an open approach utilizes the same aforementioned incisions in addition to a small hidden incision below the columella (that fleshy partition that separate the left and right nostril). The open approach allows me to see both the left and right nasal tip cartilages simultaneously so that any maneuver I would perform on the other can be immediately assessed with its opposite counterpart. Sutures are meticulously placed in a strategic fashion in order to change the shape of the cartilages from a round convex shape into more of a triangular one which, in turn, will translate to a more refined, elegant nasal tip. Think of assembling a ship in a bottle via strings, so to speak. The rhinoplasty surgeon cannot just bend cartridges, he must utilize sutures in order to shape them. This is part of the stock-in-trade of nasal tip/nasal cartilage manipulation. |
||||||||||||||
|
||||||||||||||
| Of course, some cartilage is removed as the surgeon sees fit. The importance of not being too aggressive cannot be overemphasized since doing so could result in an unsightly “pinched tip”. Finally, it is more often than not necessary to “defat” the under surface of the thick sebaceous nasal skin that would accompany such a bulbous tip. This allows the thick “sleeping bag” to redrape more fluidly over the newly reconstructed nasal cartilages.
Swelling of the nose may take many months to even a couple of years to fully disappear. This does not mean that the patient would not enjoy the effects of a rhinoplasty before then. It is just that the skin can remain slightly swollen for prolonged periods of time. The last area for swelling to dissipate is at the nasal tip area. So even though great of a 95% of my patients love their nose at the 21st day postoperatively, some will say that they would like their nasal tip to become further defined. I may either inject some Cortizone underneath the skin to turbocharge the swelling to go away quicker or just recommend patients. Sometimes that’s the hardest thing for inpatient to digest. For more information, click here and here See the following example: |
||||||||||||||
|
||||||||||||||
|
Another example of an isolated bulbous tip with thin skin: |
||||||||||||||
|
||||||||||||||








Eradication of Horizontal Neck Lines
Dr Randal Haworth of Beverly Hills had discovered an incredibly effective way of diminishing those troublesome horizontal neck lines.Only until recently has an effective method to erase horizontal neck lines or groves if you will been developed. Plastic surgeons have only offered neck lifts as a way to smooth these lines out and despite their efficacy in restoring youthful jawline and correct a “turkey neck”, they feel short in terms of treating those aging horizontal neck lines. As an alternative Botulinum toxin (Botox™, Dysport™, Xeomen™) can be injected into the platysmal bands of the neck and though it can “lift” the neck and lessen the aging cords of the neck, it does little to nothing to remove the horizontal lines. I have found that judicious use of a filler strategically injected under magnification into the precise layer below the horizontal grooves can dramatically decrease or even erase the stubborn lines. I usually start with a temporary filler such as Juvederm™ or Radiesse™ and once the patient is satisfied, I can then graduate to a permanent filler such as Artefill™., one the former substances dissipate . Here is a typical example of a before and after of a filler to the horizontal lines to the neck: |
||||||
|
||||||


10% weight loss in 10 days
Dr Randal Haworth of Beverly Hills discusses one of the most effective diets to hit the US.
Yes, it is true. Men can lose up to 10% of their total body weight in 10 days while women can lose up to 7%!I have been so impressed with the results that I am now offering this weight loss program at The Haworth Institute in Beverly Hills as part of our commitment to not only human aesthetics but also health and well being.
These results are achieved with what nutritionists and other scientists refer to as a ketogenic diet, one in which only body fat and no muscle mass is lost. Pure liquid protein is fed via a minute clear feeding tube and this, in turn, induces one’s body to first burn off the 48 hour glycogen reserve within the liver, after which time the body re calibrates itself to burn off pure fat. During this process, ketones are concomitantly released and expelled in the urine (which can be measured via dip “sticks” we provide), indicating that the body is in ketosis and fat is being efficiently burned.
The diet is divided into cycles, each of which last 10 days. As aforementioned, men can lose 10% of the body weight within one cycle while women can lose 7%. After a diet phase is complete, the patient is referred under the guidance of our nutritionist. After 10 days, a second cycle of the 10 Pro-Ten may be initiated during which time men can lose another 10% while women can lose, not 7, but 10% of their body weight .
Think of it-after 30 days, a patient can lose an unprecedented 20% of their total body weight. By way of example, a 200 lb man will lose 20 lbs after 10 day cycle then , after waiting 10 days may lose another 18 lbs (10% of 180 lbs),resulting in a total weight loss of 38 lbs in 30 days!.
To get started on this program, Dr Haworth or one of his associates will evaluate your suitability for the 10 Pro-Ten diet and , if you are deemed eligible, then some basic blood tests are drawn for analysis. Once cleared, the patient has a micro feeding tube inserted via the nose into the stomach. This sounds far worse than it is. There is virtually no discomfort with this very quick maneuver. The tube is then connected to a mini high-tech pump which infuses the protein mix and a constant rate, 20 hours a day. This pump and associated protein are situated within a small backpack which one carries around with them for the 10 days of the cycle. One can detach the tube from the pump in order to shower or exercise.Sleep should not be a problem.
There is little to no hunger with this program thus minimizing any temptation to “cheat”, unlike conventional dietary regimens.
To summarize the advantages of the 10 Pro-Ten diet:
Yes, it is true. Men can lose up to 10% of their total body weight in 10 days while women can lose up to 7%!I have been so impressed with the results that I am now offering this weight loss program at The Haworth Institute in Beverly Hills as part of our commitment to not only human aesthetics but also health and well being.
These results are achieved with what nutritionists and other scientists refer to as a ketogenic diet, one in which only body fat and no muscle mass is lost. Pure liquid protein is fed via a minute clear feeding tube and this, in turn, induces one’s body to first burn off the 48 hour glycogen reserve within the liver, after which time the body re calibrates itself to burn off pure fat. During this process, ketones are concomitantly released and expelled in the urine (which can be measured via dip “sticks” we provide), indicating that the body is in ketosis and fat is being efficiently burned.
The diet is divided into cycles, each of which last 10 days. As aforementioned, men can lose 10% of the body weight within one cycle while women can lose 7%. After a diet phase is complete, the patient is referred under the guidance of our nutritionist. After 10 days, a second cycle of the 10 Pro-Ten may be initiated during which time men can lose another 10% while women can lose, not 7, but 10% of their body weight .
Think of it-after 30 days, a patient can lose an unprecedented 20% of their total body weight. By way of example, a 200 lb man will lose 20 lbs after 10 day cycle then , after waiting 10 days may lose another 18 lbs (10% of 180 lbs),resulting in a total weight loss of 38 lbs in 30 days!.
To get started on this program, Dr Haworth or one of his associates will evaluate your suitability for the 10 Pro-Ten diet and , if you are deemed eligible, then some basic blood tests are drawn for analysis. Once cleared, the patient has a micro feeding tube inserted via the nose into the stomach. This sounds far worse than it is. There is virtually no discomfort with this very quick maneuver. The tube is then connected to a mini high-tech pump which infuses the protein mix and a constant rate, 20 hours a day. This pump and associated protein are situated within a small backpack which one carries around with them for the 10 days of the cycle. One can detach the tube from the pump in order to shower or exercise.Sleep should not be a problem.
There is little to no hunger with this program thus minimizing any temptation to “cheat”, unlike conventional dietary regimens.
To summarize the advantages of the 10 Pro-Ten diet:
- Fat loss, not muscle
- Relative low cost
- No surgery
- Very safe
- Little to no hunger, thus maximizing compliance
- Last but not least, extremely effective with up to 10% body weight loss in 10 days
The one disadvantage is the feeding tube but experience from Italy (where this concept was popularized) reveals a very high patient satisfaction rate for both “obese” patients and those requiring a small “tune up” before a special occasion, the holidays or a photo shoot whereby a patient needs to lose a certain amount of body fat quickly and safely. Cost for a 10 day cycle approaches $1500.00 at the time of this writing.
For further information call 310 273 3000
The Classic Reduction Rhinoplasty
|
As a primary and revision rhinoplasty specialist, Dr. Randal Haworth of Beverly Hills excels with all types of complicated nose jobs, but sometimes it is a simple pleasure to be confronted with a classic reduction rhinoplasty. Though these are relatively simple in concept, all nosejobs (or rhinoplasties) must be handled with utmost care and dedication to excellence.
Why does a prospective patient consult with me requesting a nosejob?
Well, most come to me with the latter concerns such as: “Doc, my nose is just too big for my face”, “I always hated my hump”, “My tip is falling like a bird’s beak”, etc., etc. Upon examination, the nose will usually manifest the aforementioned undesirable characteristics to varying degrees:
Check out this patient, who underwent a classic reduction rhinoplasty on the Swan. Here is a typical example of a classic reduction rhinoplasty,even though only subtle changes were performed. Note that a radix graft (to raise the nasal frontal angle) was placed to add height and therefore elegance to her nose. For a more general overview of rhinoplasty, go to: http://www.drhaworth.com/rhinoplasty/ |
||||||||
|


Botox for wrinkles, lips, necks and more….
I have been using Botox™ for close to 16 years now and have successfully applied it to not only erase forehead and eye region wrinkles, but also to improve the oral area and neck. By strategically injecting small amounts of Botox™ into the upper lip I can help curl out the upper lip by emphasizing the “white roll” or vermillion border as well as soften the stubborn wrinkles there. Also I can elevate the otherwise sad, downturned corners of the mouth by injecting into the depressor anguli oris muscle (DAO) and produce a minor facelift by injecting the platysma muscle of the neck.
The chin can also by smoothed out by ridding it of that aging cobblestone appearance when grimacing, while pore size can be reduced by selectively placing Botox™ into the dermis of the skin only. With this latter technique (when injected into the forehead), the patient can still move their brows but their wrinkles are vastly reduced as well as their pore size- that frozen look is avoided which is especially important for my actor patients. Xeomen™ is a new substitute for Botox and has a number of advantages.
For further information, check out these Extra™ LifeChanger features on the very subject:
The chin can also by smoothed out by ridding it of that aging cobblestone appearance when grimacing, while pore size can be reduced by selectively placing Botox™ into the dermis of the skin only. With this latter technique (when injected into the forehead), the patient can still move their brows but their wrinkles are vastly reduced as well as their pore size- that frozen look is avoided which is especially important for my actor patients. Xeomen™ is a new substitute for Botox and has a number of advantages.
For further information, check out these Extra™ LifeChanger features on the very subject:
The Injectable Nosejob
In the era of Twitter, Facebook, texting, rapid- fire music video editing, etc. everyone (including those not diagnosed with ADD) wants instant results. So what is unusual with wanting an instant nose job or rhinoplasty? Absolutely nothing. An instant nosejob is performed by strategically injecting a pre-chosen filler just below the nasal skin in an aesthetically sensitive manner. Temporary fillers such as Hyaluronic acids (Restylane™, Perlane™, Juvederm™, etc.) and calcium hydroxyappatite (Radiesse™) may be used as a “dress rehearsal” to confirm if the patients like their result. If so, many will then opt for a more permanent filler, either in the form of fat, Artefil ™ or Aquamid ™ (which is not yet FDA approved).
The appeal is obvious: less bruising, less prolonged swelling, less initial expense, less scary for the wary and more predictable (in the proper hands) with less risks. However, the injectable technique cannot be used to correct all types of cosmetic nasal problems and deformities. This is especially true for noses that need to be reduced in size and refined in shape. One does not need to be a genius to realize that fillers may do little to make a nose smaller by removing humps, refining tips and narrowing bones, no matter how well injected they are. The ideal candidate for an injectable rhinoplasty is the nose that needs to be augmented, either via it’s bridge (or dorsum) or it’s tip or both. A drooping tip can be elevated only to a subtle degree with filler.
Filler is also a great solution to those noses that have minor irregularities stemming from prior rhinoplasties. Filler will generally not help breathing problems. To learn more about this elegant solution to a rather common problem, check out these videos:
1.Extra Injectable NoseJob
2.Today Show Injectable NoseJob
3.Extra Artefill Injectable revision rhinoplasty
Dr Randal Haworth of Beverly Hills counts primary and revision rhinoplasty as one of his specialties of plastic surgery
The appeal is obvious: less bruising, less prolonged swelling, less initial expense, less scary for the wary and more predictable (in the proper hands) with less risks. However, the injectable technique cannot be used to correct all types of cosmetic nasal problems and deformities. This is especially true for noses that need to be reduced in size and refined in shape. One does not need to be a genius to realize that fillers may do little to make a nose smaller by removing humps, refining tips and narrowing bones, no matter how well injected they are. The ideal candidate for an injectable rhinoplasty is the nose that needs to be augmented, either via it’s bridge (or dorsum) or it’s tip or both. A drooping tip can be elevated only to a subtle degree with filler.
Filler is also a great solution to those noses that have minor irregularities stemming from prior rhinoplasties. Filler will generally not help breathing problems. To learn more about this elegant solution to a rather common problem, check out these videos:
1.Extra Injectable NoseJob
2.Today Show Injectable NoseJob
3.Extra Artefill Injectable revision rhinoplasty
Dr Randal Haworth of Beverly Hills counts primary and revision rhinoplasty as one of his specialties of plastic surgery