Blessed with gorgeous looks, Jesinta Franklin (née Campbell) was crowned Miss Universe Australia back in 2010. Dr. Haworth told Daily Mail Australia that he ‘strongly suspects’ Jesinta has had a brow lift and that it ‘appears as if she has had a rhinoplasty’ in order to enhance her natural beauty. Dr. Haworth observed that Jesinta ‘now possesses a near-perfect classical balance of facial features’ and believes a subtle brow lift may be behind the change. ‘I strongly suspect that she had a brow lift of some sort, either done with strategic Botox injections or, more likely, with surgery,’ he said.
Dr. Haworth believes that from certain angles ‘it appears as if Jesinta had a rhinoplasty to define her tip and narrow her nasal bones’. He explained that, if Jesinta has indeed gone under the knife, the results are striking yet subtle. Daily Mail Australia contacted Jesinta’s management for comment, who described the claims as ‘ridiculous’. Jesinta has previously spoken about her decision to have a breast enlargement as a teenager. ‘It’s a personal choice and completely up to the individual,’ she said at the time. ‘When I was young I had a small procedure done to become a 12B.’
As trifling as it may seem to the layperson, aesthetic surgery is serious business. Apart from obvious cosmetic ramifications, the seriousness becomes understandable when one considers that the surgeon must first make a healthy patient temporarily unwell in order to make he or she look better in the end. It is for this very reason plastic surgeons have an added unique responsibility which surgeons of other specialties simply do not bear. Choosing to undergo elective surgery is a series of decisions made by both the surgeon and the patient. As with all aspects of medicine, nothing is absolute, it is about controlling probability.
In this day and age, patients increasingly view plastic surgery as nothing more than a haircut with a short recovery, let alone one with a complication. Even under the best of hands, a complication can arise for any number of reasons and if it does, acting as a team with your surgeon is crucial. Whether following a facelift, rhinoplasty or any plastic surgery for that matter, almost all complications can be fixed in the end, even if multiple surgical revisions are needed.
It is normal for the layman to consider surgical results as either “good” or “bad”, but those adjectives can be misleading and are certainly inadequate in revealing the true story behind the result.
“Good” surgery with a complication is not the same as “bad” surgery per se. In other words, complications do not all come from “bad” surgeons and indeed, “bad” surgeons may have successfully completed an operation without encountering obvious complications. I think it fair to say most patients consider themselves as good people and if a complication happens to them, they will perceive themselves as victims of a bad surgery and by extension, a bad surgeon. So what is the difference between “bad” surgery and a “good” surgery with a complication?
Look at it this way… in any profession, there are the “good”, the “bad” and the “excellent”. For the sake of this discussion, let’s just oversimplify the comparison between “good” and the “bad”. Since plastic surgery is as much an art (or at least an artisanal craft) as it is a science, whereby results are measured both objectively and subjectively, it is not unreasonable to compare a plastic surgeon to any artist or craftsman, including sculptors, painters and woodworkers. Artists filter their talent and vision through years of experience to not only earn but continually solidify their reputation as either being “good” or “bad”. Moreover, good artists become respected by not just producing one “good” piece but doing so consistently, whereas the “bad” consistently create sub par results as judged by the median consensus.
However, all artists, whether good or bad, are limited by the quality of material with which they work. It is known that Michelangelo’s David has been deteriorating at a far more rapid pace than would be expected because of the poor quality of its marble composition. Bernini also broke a piece of marble in half through chiseling into an unexpected vein in the stone causing him to start all over with a brand-new block. Does that make him a bad artist? Hardly not.
In other words, complications happen and that’s why there are consents to protect not only the doctor but also the patient. Consents should ensure the patients are informed as to the shared risk both they and the surgeon take when undergoing surgery.
Many complications are avoidable. Both doctors and patients must do their part to optimize a certain outcome and minimize the risk of complications. Patients must avoid certain medications that may promote bleeding, cease all smoking for optimal circulation, follow instructions and take medications as prescribed. Otherwise, surgery may be self-sabotaged. On the other hand, surgeons must do their part in educating and performing the proper operation in the right patient with skill and dedication.
Other complications are unavoidable and just because they may be explainable in hindsight does not mean they were avoidable within the context they occurred. This is why it is paramount that patients disclose all of their medical history and follow their surgeon’s instructions to a T in order to minimize unexpected situations such as abnormal bleeding, poor wound healing, etc..
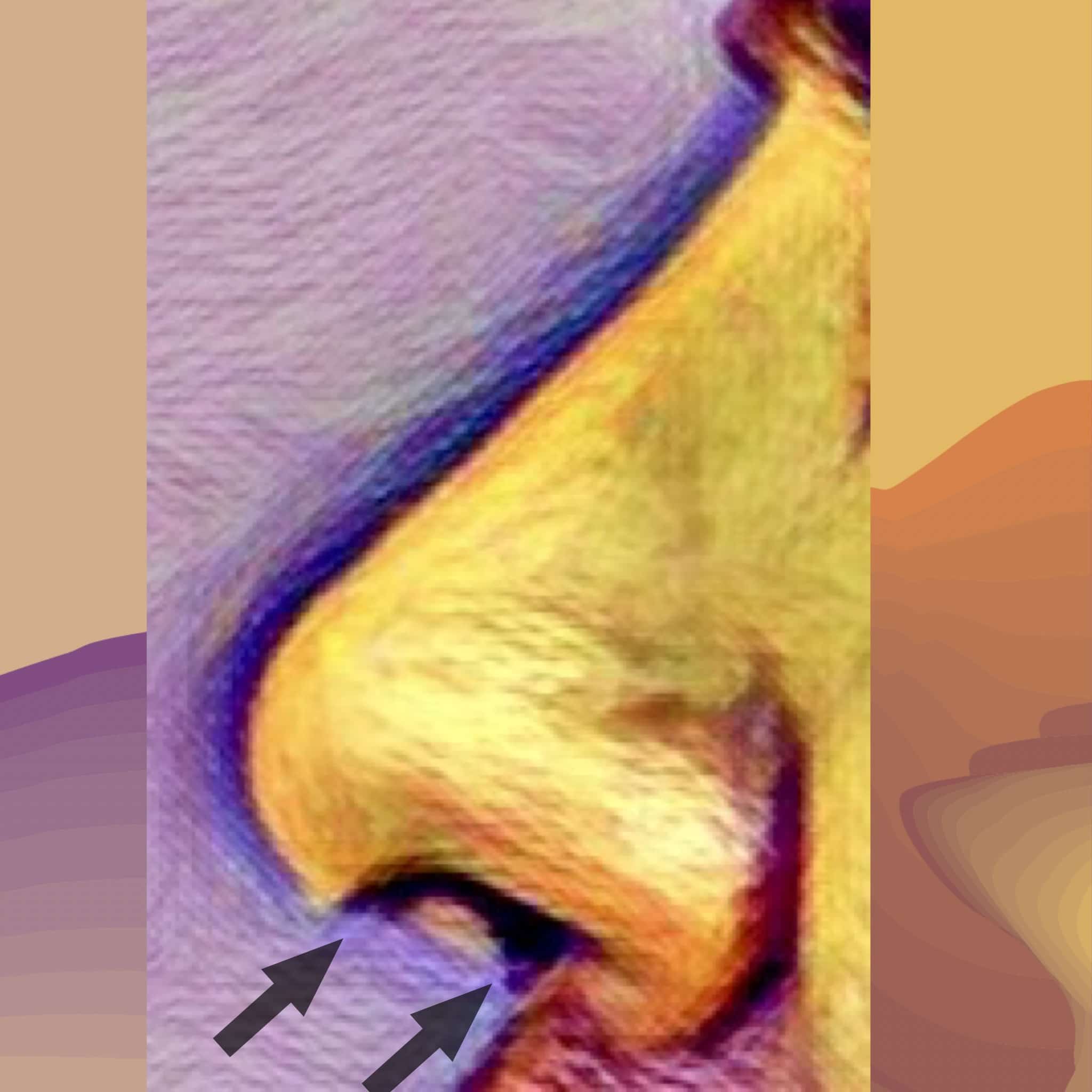
What spurred me to write this particular blog was a recent experience having performed a complex revision rhinoplasty on a dear friend of mine of 20 years. Unfortunately, this advanced detailed nasal reconstruction was exacerbated by unexpected physiological conditions including excessive bleeding and poor tissue characteristics. The next day, the patient presented with so much swelling underneath the pressure cast that it was being pushed off the face. The swelling was a hematoma which I immediately evacuated from under the skin (it was 4 1/2 mL, being the largest nasal hematoma encountered by either my colleagues or myself). Accompanying this was necrosis (death) of the columellar skin (the partition separating his left and right nostrils). This was particularly disappointing to say the least because the surgical results in terms of nasal shape, symmetry, tip definition and projection were otherwise excellent. Yet losing coverage over the columella would have serious ramifications.
Despite attempts to bring vascularized tissue using local intraoral flaps, my friend eventually needed the help of a certain specialist to bring fresh tissue to the columella below the nasal tip with a temporary forehead flap.
The arrows on the drawing illustrate that portion of the nasal skin (overlying the columella) that was necrotic. Replacement is required through vascularized tissue flaps
Albeit exceedingly rare, this 1.5 x 1.2 cm skin loss was enough to eradicate not only their trust in me as a surgeon but also our long term friendship. Most patients understandably experience a spectrum of emotions including panic, sadness, denial, anger and ultimately acceptance from a complication such as this. However, nothing could prepare me for the degree of ongoing vengeful anger and hostility the patient and their partner have directed towards me including threats to go to the press and ruin my reputation.
Anger is not only destructive but also lacks focus, therefore it can be especially counterproductive to both healing and a good result (not to mention friendship!). Premature castigations of blame fuel brash, illogical decisions which actually complicate the original complication.
Understanding the differences between “bad” and “good” surgery and “good” surgery with a complication can certainly help put things in perspective. When a patient concedes the net surgical aesthetic result, at least in terms of shape and symmetry, as good if not excellent, he or she is less likely to question, and more likely trust, their original choice of surgeon. Whether their breast lift incision opened or, as in this case, a small but strategic portion of nasal skin died, the affected patient will see the “bigger picture” and believe their surgeon will do the right thing by having their best interests at heart. This same patient understands that they were not necessarily a victim or unjustifiably punished by “bad” surgery. Instead, they will accept things for what they are, learn patience and develop a sense of optimism to set themselves up for the best possible outcome in the future.
The majority of complications concern wound healing and minor infections. For these, possible antibiotics and the “tincture of time” for healing to occur are required. Other times, simple, clinical interventions such as laser treatment, injections, the occasional scar revision and creams are all that are needed.
Other complications require more invasive solutions. Depending on the type of complication, an expeditious trip to the operatory maybe all that is required (e.g.,to drain a hematoma) whereas staged surgical revisions may be undertaken in the extremely rare case of tissue loss.
Most surgeons will recognize if a particular complication is beyond their level of expertise. A patient should not feel abandoned or simply passed off if they are referred to another expert if a complication warrants it. It is important to recognize that medicine is team work and the referral is simply a reflection of the original surgeon’s dedication to the best outcome possible.
Emotional advice after a complication
–Watch out for advice with an agenda. It is understandable that if a complication does arise, fear and anxiety will prompt you to seek solace and advice from friends and family members. While this is wholeheartedly encouraged, it is important to remember that not all the advice given is good especially considering that those giving advice are not often doctors nor do they know the intricate details of the patient’s particular case. Though most advice is well-meaning in intent, some may be motivated by guilt, jealousy, personality disorders or just plain ignorance. Furthermore, the advice a patient may obtain from elsewhere may be counterproductive because it may only increase their level of anxiety.
–Stay optimistic and avoid jumping to any pessimistic conclusions. It is not unheard of that acute anxiety will provoke a patient to impatiently reach for the help of an alternative plastic surgeon. Unfortunately, some plastic surgeons may be unscrupulous and advise the fragile, highly suggestible patient into unnecessary and ill-timed surgery claiming it is urgently needed to prevent some permanent deformity. Always keep a line of communication open with the original plastic surgeon to not only help allay personal fears but also be guided in the right direction with a second opinion if necessary.
New techniques always emerge which supplant the old. The same is true with the plastic surgical procedure called rhinoplasty, or in common parlance, nose job. A nose is basically composed of three materials: overlying skin with associated fat, bone and cartilage.
A rhinoplasty involves:
changing the shape and slant of the bones through selective filing and cutting
changing the shape of the cartilages through removal, adding and reshaping with sutures and
in selected cases, “defatting” the skin to allow the shape of the cartilages and bone to “shine through”.
In order to perform the rhinoplasty, the surgeon must gain access to the underlying bone and cartilage through either through a closed or open technique. The former involves making incisions confined to within the nostrils and performing the surgery through the limited exposure that these incisions thus provide. The latter, open technique, involves making the same incisions within the nostrils but joining them across the columella (the fleshy partition that separates the left and right nostril at the base of the nose).
I am frankly surprised and amused that in 2017, some plastic surgeons still insist that the closed technique, when “performed properly”, provides equal or even superior results than those obtained with an open one. These same surgeons cite a few old masters of closed rhinoplasty fromthe 1970s and 80s to support their contention that the closed method is superior. However, the best results from these old Masters do not parallel those obtained from top rhinoplasty surgeons today. Whether you like it or not, progress is inevitable and the new masters of today produce better results than the masters of yore.
I recently attended two conferenceshosting some of the top thought leaders in rhinoplasty surgery. As expected, there was not one expert in the room who would consider closed rhinoplasty an option to achieve the delicate and precise results expected by their patients. Indeed, even in their hands they felt that a closed rhinoplasty generally leads to a subpar result. Imagine having to work on the engine of your car only through the left and right front wheel wells. Without opening the hood to gain full unimpeded access to the engine, your ability to effectively work is exceedingly hampered.
The results of any plastic surgery should be measured by the end visual result and not by the process to achieve it.
Those who promote closed rhinoplasty as better invariably cite less swelling and no potentially visible scar as their main selling point, but this is a fallacious argument. When properly performed, as a top Beverly Hills rhinoplasty expert, Dr Randal Haworth has seen minimal to no difference in postoperative swelling between the open and closed methods and the scars essentially become invisible whether you are a young model or a 70-year-old person. The proponents of closed rhinoplastyproudly display their early smooth and symmetrical resultsas being superior. However, in the early postoperative period, it is the very swelling that the closed proponents claim is not there that may be masking inaccurate nasal construction below. This can be seen in the many examples of famous nosesheralded in their early postoperative period but turn out poorly constructed when their swelling dissipated. Generally avoidable deformities such as inverted V deformities, pinched tips and crooked noses become unavoidably visible no matter how much makeup contouring and good lighting is available.
Famous Noses and Deformities via Closed Techniques:
After closed rhinoplasty with obvious ‘inverted V” deformity, pinched tip and lack of harmony between the upper and lower portion of the noseNote the lack of continuity between the upper bony portion of the nose and the lower cartilaginous portion. An obvious “inverted V” deformity and pinched tip do not help the situation.After a closed rhinoplasty, note crooked appearance, asymmetrical and drooping pinch tip
Examples of Complex Rhinoplasties Performed through the Open Technique:
Significant congenital asymmetry of the nostrils. After an open rhinoplasty-note significantly improved symmetry with minimal scar that a closed rhinoplasty technique can’t achieveUnfortunate result from a closed rhinoplasty with “inverted V” deformity and asymmetrical, bulbous tip. An open rhinoplasty was performed with significant improvement of the noseUnfortunate result from a closed rhinoplasty with “inverted V” deformity, retracted nostrils and asymmetrical, bulbous tip. An open rhinoplasty was performed with significant improvement of the noseUnfortunate result from a closed rhinoplasty with “inverted V” deformity, retracted nostrils and asymmetrical, bulbous tip. An open rhinoplasty was performed with significant improvement of the noseAnother example of noticeable congenital asymmetry of the nostrils. After an open rhinoplasty-note significantly improved symmetry with minimal scar that a closed rhinoplasty technique can’t achieve
When precise control over the shape and symmetry of the nose is required as well as control over the subtle light reflexes and shadows embodying the beauty of a nose, nothing beats an experienced surgeon with a precise touch, an aesthetic sensibility and an open rhinoplasty technique.
Very few surgeons in the world understand aesthetics to the point where they can be a true hyperaesthetic facial plastic surgeon specialist. A hyperesthetic specialist is similar to the conductor of an orchestra-he or she needs to know all the instruments better than the individual players in order to “orchestrate” them to create melodious harmony without dissonance. One of the keys to create visual harmony in the face is mastering lip rejuvenation surgery-it’s not just about adding volume (which is essentially what most practitioners and patients equate with lip enhancement), it’s about mastering the shape of both the upper and lower lip. Patients travel from all corners of the globe to top Beverly Hills plastic surgeon and lip augmentation specialist, Dr Haworth to undergo hyperesthetic change, which may include any number of surgical art performances including a high-profile facelift, endoscopic brow lift, blepharoplasty, rhinoplasty or his lip reshaping signature surgery! https://youtu.be/cI3nEq5R3x8
Wier excisions are very powerful tools to augment a rhinoplasty. This is a procedure that I usually perform at the conclusion of a nose job in order to refine and narrow the nostrils while controlling the flare when smiling.
Most people and surgeons alike equate this procedure to simply narrowing the “floor” of the nostril by cutting out some skin but it is actually more nuanced than that. The design of the excision can be customized by changing the angulation, the position and the width of the cuts which, in turn, can change not only the dimensions but also the curvature of the actual nostril itself. A deep permanent suture is often used as well to prevent re-widening of the nostrils and reduce tension across the scar. Reducing tension across the scar as well as accurate angulation is important to achieve a nearly invisible scar. So many times I have seen obvious notching that is visible from 5 feet away and is a definite giveaway of having had a rhinoplasty.
Weir excisions can be also be performed in conjunction with an upper lip lift adding to the complexity of the procedure. As a rhinoplasty and lip lift expert, I have performed hundreds of these combination techniques with excellent results.
All facial plastic surgery, whether it’s primary or revisional, is challenging but taking the time to address all the details and plan them accordingly can maximize the aesthetic outcome that is not only beautiful but natural as well. The devil is in the details so to speak.
Poor rhinoplasty result with crooked , distorted tip and obvious nostril scarring after a Weir excisionAgain, note obvious nostril scarring from Weirs and tell-tale signs of a past rhinoplastyBefore and after revision rhinoplasty and Weir excision as performed by Dr. RANDAL HAWORTHPrimary rhinoplasty and Weir excision to narrow the nostrils in Asian patient. Note added tip projection and lack of notchingPrimary rhinoplasty, Weir excision and concomitant upper lip lift as performed by Dr. Haworth
By trade-offs, I am not referring to complications or risks.
By trade-offs I am referring to subtle and sometimes significant alterations in your appearance that will be incurred by undergoing a certain plastic surgical procedure. It is the doctor’s responsibility to inform the patient of these trade-offs (including risks of complications) while it is the patient’s responsibility to make an informed decision to proceed if he or she feels that the benefits of the surgery will outweigh the risks and trade-offs.
Examples of such trade-offs are the scars in and around the ear that result from a facelift. Even though they may be near invisible, they are scars nonetheless. The majority of patients feel that benefits of the facelift outweighed any of the associated trade-offs. Similarly, patients who undergo an abdominoplasty (tummy tuck), mastopexy (breast lift) or brachioplasty (arm lift) should be fully aware that they will develop scars from those procedures. Though the majority will heal well with very acceptable scars, most of the time the scars will be visible to some degree.
Patients who undergo a rhinoplasty must understand that their nose will be numb, stiff and hard for up to 3 months or more while swelling can persist for 1 to 2 years. Numbness from a facelift or a browlift can last many months as well. Despite understanding these trade-offs, the vast majority of patients have no problem undergoing these procedures once they have decided to do so.
Over the years, I have found it curious that a small minority of patients undergoing lip reshaping surgery in the form of upper lip lifts and V-Y plasties had unrealistic expectations in terms of their healing and results. They were surprised even angry that they experienced numbness, stiffness and associated scarring. Sometimes a very subtle change in the nostril position occurred after the surgery. These trade-offs may arise even though the result of the upper lip lift is successful from the aesthetic standpoint-in other words, the net benefit in the sensual-youthful-beauty quotient for the face has been increased. However, a few may consider the lip lift a failure if they have experienced even a slight degree in any of these trade-offs.
Though these trade-offs can mostly be successfully reversed, a patient should not elect to undergo such a procedure if he or she will not accept that these can be normal aspects of the procedure. If one thinks about it, an upper lip lift will have its trade-offs in the same way other procedures would have their own yet it perhaps gets more attention than other anatomical features of the face because the lips are expected to not only look beautiful but also function as well.
And function they do, more than any other part of the face. Indeed, lips are used to express, emote, eat, kiss and speak-essentially they move millions of times a day! Because of these strong repetitive muscle forces around the nasal and oral region the plastic surgeon must create a strong upper lip lift that will resist these forces in order to achieve a result that is long-lasting, with minimal scarring and nasal distortion.
In fact, lip shaping procedures are the most challenging of all facial plastic surgeries, even rhinoplasties. Though the success of facelifts are measured in centimeters, brow lifts in increments of 2 to 4 mm and rhinoplasties in millimeters, lip reshaping surgery is measured in quarter-to-an-eighth of a millimeter! With those scales, one can almost consider this close to microsurgery.
In 2014, it would be a miracle to undergo an upper lip lift with an unequivocal guarantee of no scarring, nasal distortion, prolonged minor sensory changes and stiffness. If you are contemplating undergoing an upper lip lift but will not tolerate any of these tradeoffs, I suggest you avoid the procedure altogether and wait for that miracle to happen.
“Plastic surgery won’t make you happy, but it can make you happier”
I think most sentient human beings will agree that the world it’s becoming a crazier place in which to live. We are constantly bombarded by negative imagery, negative stories, negative experiences, negative people while reminded that we are not good enough to fit the ideal as embodied by the media’s ambassadorial cadre of celebrities and certain reality stars. In more recent years, I am seeing an uptick in the amount of negative patients in my practice. I have learned to better recognize them and avoid operating on them as best I can.
Why do I do this?
The answer is simple. I avoid operating on them to better serve them . My staff and I at the Haworth Institute adhere to a basic principle of delivering the best service possible in order to maximally satisfy our patients. Yet, even if I perform the most exemplary plastic surgery and the patient is not happy with the results, then I have failed. In other words, the objective assessment of the surgical results does not match the subjective one of the patient. There are reasons for this break from reality, such as body dysmorphic syndrome and a patient’s own internal anger, discontentment, strife or call it what you will. There is much written about body dysmorphia but little is discussed about the latter situation-the angry, malcontent. Many times, these people come to a plastic surgeon seeking out surgical transformation for the wrong reasons, thinking that the surgery itself will bring a positive change in their life. When that doesn’t transpire and the patient realizes that they are still the same unhappy soul, all hell can break loose for both patient and caregiver because of unrealistic expectations. This may become a greater incendiary situation when a patient is taking Adderall or some other amphetamine-related prescription medication. Consequently, plastic surgeons should be aware of this heretofore anecdotal correlation prior to operating on anyone taking Adderall or equivalent since this may be a predictor of both disproportionate patient disappointment and anger.
I now have come up with the following saying within the last month which resonates with both my staff and myself: “Plastic surgery will not make you happy, but it can make you happier.” In simple terms, this allows me to assess whether a patient is fundamentally happy and balanced prior to operating on them. I’m sure that there will be a few patients that still slip through the cracks, so to speak, but if I can manage to avoid operating on the majority of angry, unhappy patients then I know in my heart that I did serve them well.
Coincidently, this article just came out today about plastic surgery and happiness:
Dr. HAWORTH is a board-certified (American Board of Plastic Surgery) plastic surgeon located in Beverly Hills. His specialties include all aspects of aesthetic facial and breast plastic surgery, including rhinoplasty, revision rhinoplasty, facelifts, lip reshaping and breast augmentation. For further information go to drhaworth.com
The Challenging Question in Modern Plastic Surgery
“I am fearful about plastic surgery. “Whenever I am in , Beverly Hills, LA or New York, I see people with bad work looking so fake. Their lips are and breasts are so out of proportion!”
I , as a Board Certified plastic surgeon in Beverly Hills, hear this time and time again in conversation at dinner or in my clinic. “I don’t want to look like Michael Jackson!” is another common proclamation of patients during nasal surgery consultations. Instead of getting frustrated with these opinions, I agree with them. It is because I understand their source. It is simple; “good” plastic surgery is invisible, while so called “bad” plastic surgery is not.
Bad plastic surgery (whether it be a rhinoplasty, facelift or breast augmentation) can result from any of the following three scenarios. The first is poor performance of a procedure. Fortunately, this is a rare occurrence when a properly trained surgeon certified by the American Board of Plastic Surgery performs the surgery. The second is poor healing by the patient, perhaps complicated by infection. Again, this is infrequent especially in healthy, well-selected patients. Finally, the third issue is the question of aesthetic taste. No amount of plastic surgical training will guarantee appreciation of balanced facial form and pulchritude. By way of analogy, not all self-professed artists who attend the same art school will emerge as equally talented artists.
What makes for good plastic surgery then? It is the fruit of a surgeon who’s not only technically proficient, but also possessive of a keen eye and aesthetic sense. A beautiful and youthful face reflects visual harmony between facial structures. With age, harmony turns into visual dissonance as youth cues disappear. As a surgeon, it’s my job to serve as a conductor to bring these diverging aging elements together again. Youth cues are lost as wrinkles, folds and sagging facial features arise. Most plastic surgical training emphasizes the re-establishment of major youth cues while overlooking the minor ones. In order to re create the major youth cues, I eradicate jowls; I soften the nasolabial folds, (the fatty accumulation that runs from the bottom corner of the nostril to the corner of the mouth,) contouring a strong jaw line and a firm neck and rejuvenating the eyelids through a combination of endoscopic brow lifting and blepharoplasty (eyelid tucks.)
In order to paint a convincing portrait of somebody in their youth, the surgeon should not only recreate the major youth cues, but also the minor ones. To do so, the surgeon must address the hollows underneath the eyes, the drooping corners of the mouth, the elongated upper lip (hiding the upper teeth), the sagging lower lip (exposing the lower teeth) and the elongated ear lobes. True visual choreography is required.
I’m excited by the array of minor youth cue procedures now developed. Most are relatively minimal in scope. Among these are the Endotine ST and B mid-face lift, the first vertical and reliable mid-face lift that not only addresses the hollows under the eyes, but also softens the nasolabial folds. All in all, it provides a more natural and subtle rejuvenation, avoiding that “pulled back” look. The procedure takes forty minutes when combined with a blepharoplasty (“eyelift” ). This technique is made possible by the development of a new absorbable device placed via the eyelid to elevate the cheek fat pad back to it’s position of youth.
There are other minor youth cues and I address them as well – by performing upper lip lifts with a hidden incision inside and around the nose, as well as corner lip lifts and earlobe reductions as necessary. The upper lip lift shortens the distance between the nose and the lip, allowing the upper teeth to be seen. One only has to peruse the fashion magazines to see how this look is indicative of a fresh and youthful lip region.
The before and after photos included below, are good examples of the above principals put to use. This 28-year-old girl has premature signs of aging from massive weight loss. Both major and minor youth cues need to be established to achieve harmonious balance. Consequently, I performed an endoscopic brow lift, lower blepharoplasties with fat transfer, an Endotine mid face-lift, liposuction of the neck, upper lip lift and fat transfer.
There are artists who have become doctors and doctors who have become artists. Since I have started painting as a little child and have graduated to exhibit my later work in respected galleries, I consider myself as one of the former. I am fortunate that my background has imbued me with an artist’s eye, which translates into my work. Regardless of Beverly Hills, New York or other urban center, Plastic surgeons should always strive to deliver to their patients not only the best technological advances in plastic surgery, but also in a way that reflects passion and inspiration with an aesthetic sensibility.
People seem to always ask me which celebrity did what and why would they do that. Sometimes that is frustrating.
A close friend of mine who is a fine art photographer tells me she can always spot if someone had plastic surgery to which I reply, “No you can’t”…
That is because good plastic surgery is invisible. Therefore, by logical extension, the only plastic surgery she or anybody can recognise is visible. Most would concur that visible plastic surgery is less ideal than invisible surgery, but this is not always the case. Think Christy Turlington and her obvious rhinoplasty as a reminder of how visible plastic surgery can elevate a face to another worldly, ethereal level and you will get my point.
Recently Extra asked me to comment what Lindsay had done to herself based on photographs.
Lindsay Lohan in better days
Lindsay Lohan in less better but recent days
This is similar to expecting a detective to know who committed a crime based solely on showing him some iPhone photos. I can only surmise what Lindsay had done. I feel assured to say she definitely had fillers in the past (just look how her lips and cheeks have changed over the years) and a breast augmentation. But recently, the poor woman has undergone more severe change and not for the better.
She looks swollen and has an obvious “double chin”. This to me is a salient clue –
1. Is she simply bloated from substance abuse or withdrawal?
2. Has she gained weight for any number of reasons (in preparation for playing Elizabeth Taylor in Liz and Dick?)
3. Is she swollen after undergoing some involved facial surgery?
Who knows? I am simply a detective here and would need to visit the crime scene, so to speak. I would need to ask questions and perform an examination!
Dr Haworth has no professional affiliation with Lindsay Lohan
As a primary and revision rhinoplasty specialist, Dr. Randal Haworth of Beverly Hills excels with all types of complicated nose jobs, but sometimes it is a simple pleasure to be confronted with a classic reduction rhinoplasty. Though these are relatively simple in concept, all nosejobs (or rhinoplasties) must be handled with utmost care and dedication to excellence.
Why does a prospective patient consult with me requesting a nosejob?
Is it that their nose is asymmetrical, twisted, dented and scarred from a past rhinoplasty gone wrong?
Is it that their nose is too small for their face with a flat bridge and wide flat tip perhaps due to Asian heritage?
Is it that their nose is too wide with a bulbous tip?
Or is it that their nose is too big, with an associated hump, wide bones and big, drooping tip (especially when smiling)?
Well, most come to me with the latter concerns such as: “Doc, my nose is just too big for my face”, “I always hated my hump”, “My tip is falling like a bird’s beak”, etc., etc.
Upon examination, the nose will usually manifest the aforementioned undesirable characteristics to varying degrees:
Is there a hump? Check
Is it comprised of bone and cartilage? Check
Does the nasal tip droop (with an acute angle between the upper lip and bottom of the nose/columella) especially with smiling? Check
Is the nasal tip wide and/or bulbous? Check
Are the nasal bones wide (where they emerge from the cheeks to form the bridge)? Check
If this common checklist is mainly affirmative, then the patient will need a classic reduction rhinoplasty. In this surgery, the tip is made narrow with either tip grafts (composed of cartilage usually invisibly harvested from the patient’s own septum), strategic suturing or both. The nasal hump is either chiseled or filed down and finally the nasal bones are narrowed by delicately in-fracturing them (“breaking the bones”). If this latter maneuver is bypassed, then an”open roof” deformity may likely arise in which the nasal bridge will look artificially flat and wide itself. Therefore the nasal bones (which comprise the sidewalls of the nose) are carefully angled inwards towards the midline in order to close the open roof which resulted from the hump removal in the first place.
Check out this patient, who underwent a classic reduction rhinoplasty on the Swan.
Here is a typical example of a classic reduction rhinoplasty,even though only subtle changes were performed. Note that a radix graft (to raise the nasal frontal angle) was placed to add height and therefore elegance to her nose.

 Dr. Haworth believes that from certain angles ‘it appears as if Jesinta had a rhinoplasty to define her tip and narrow her nasal bones’. He explained that, if Jesinta has indeed gone under the knife, the results are striking yet subtle. Daily Mail Australia contacted Jesinta’s management for comment, who described the claims as ‘ridiculous’. Jesinta has previously spoken about her decision to have a breast enlargement as a teenager. ‘It’s a personal choice and completely up to the individual,’ she said at the time. ‘When I was young I had a small procedure done to become a 12B.’
Dr. Haworth believes that from certain angles ‘it appears as if Jesinta had a rhinoplasty to define her tip and narrow her nasal bones’. He explained that, if Jesinta has indeed gone under the knife, the results are striking yet subtle. Daily Mail Australia contacted Jesinta’s management for comment, who described the claims as ‘ridiculous’. Jesinta has previously spoken about her decision to have a breast enlargement as a teenager. ‘It’s a personal choice and completely up to the individual,’ she said at the time. ‘When I was young I had a small procedure done to become a 12B.’