
Author: omnispear
W (1999)
Dr. Randal Haworth , also of Beverly Hills, would provide treatment for a “complete rejuvenation,” while keeping Parker Bowles from looking plastic. Besides Camilla’s fair skin, well proportioned nose and good bone structure, “I think underneath it all she’s got nice eyes,” Haworth adds, “and I’m told that her personality is one of her strong points.”

Parade (1999)
Sally Kirkland: Bad experience with her implants
Question:
I’m tired of seeing so much cleavage at the showbiz awards shows. Has everyone in Hollywood had breast implants? What happened to the health concerns about silicone?
Answer:
“Silicone has been eclipsed by the safer saline-filled implants,” says Dr. Randal Haworth , a Beverly Hills platic surgeon who recently reconstructed actress Sally Kirkland’s breasts after complications from her implants. He thinks the desire for big breasts is related to California’s beach culture. But the tide may be changing. Former Baywatch babe Pamela Anderson had her implants removed last month, explaining: “I just wanted my natural body back.” (She was surprised to learn that one side had been leaking.)
Question:
I’m tired of seeing so much cleavage at the showbiz awards shows. Has everyone in Hollywood had breast implants? What happened to the health concerns about silicone?
Answer:
“Silicone has been eclipsed by the safer saline-filled implants,” says Dr. Randal Haworth , a Beverly Hills platic surgeon who recently reconstructed actress Sally Kirkland’s breasts after complications from her implants. He thinks the desire for big breasts is related to California’s beach culture. But the tide may be changing. Former Baywatch babe Pamela Anderson had her implants removed last month, explaining: “I just wanted my natural body back.” (She was surprised to learn that one side had been leaking.)
VOGUE (1998)
FEMME SOUTH AMERICA (1998)

LOS ANGELES – BEST OF ISSUE (1998)
BRAND YOURSELF- NONFICTION BOOK (1998) – BRAND YOURSELF- NONFICTION BOOK
You may well have seen Dr. Randal Haworth on Entertainment Tonight or other
national television programs. He is a celebrated plastic surgeon who
invented the Haworth Lip Technique, boasts a clientele of celebrities and
socialites from around the world, and was recently named one of the best
eight in his field by Los Angeles magazine.
Dr. Haworth’s office (which includes full operating facilities) is
a perfect reflection of his brand. “It is important for a plastic surgeon
to show prospective patients the aesthetic side of his personality without
going too far over the edge,” he notes. “I am, after all, a
board-certified surgeon, and would thus not want to be perceived as a
‘fringe personality.’ ”
This doctor’s office strikes an excellent balance: the reception
area is warm and welcoming, while the inner offices maintain the requisite
clinical feel. Of special note is the fact that Dr. Haworth’s own painting
are exhibited through the office and examination rooms. “Part of my brand,”
Dr. Haworth explains, “is that I am not only a highly trained plastic
surgeon, but a man with highly developed aesthetic sense. In fact,” he
continues, “I will be exhibiting my work at Bergamot Station (one of Los
Angeles’s most respected art venues) later this year. This tells patients
not only that I have a strong sense of aesthetics and composition, but that
I am a well-rounded individual, with interests that extend far beyond the
realm of my medical practice.”
BEVERLY HILLS WEEKLY (1997) – BEVERLY HILLS WEEKLY
Facial rejuvenation is like making a bed. It is a two step
process. First, one needs to start with clean, freshly ironed sheets.
Secondly, the actual bed is made by carefully draping, rearranging, folding
and finally tucking these sheets into place. The final results is a soft,
harmonious and good looking arrangement that invites company rather than
rejects it. How does this analogy applies to the face?
We need to imagine our skin as our sheets. The ideal skin should
be clean, opalescent and smooth. The skin should be relatively free of
disconcerting wrinkles and folds. The skin should be adherent to the
underlying facial structures in a natural fashion, free of redundancy and
looseness.
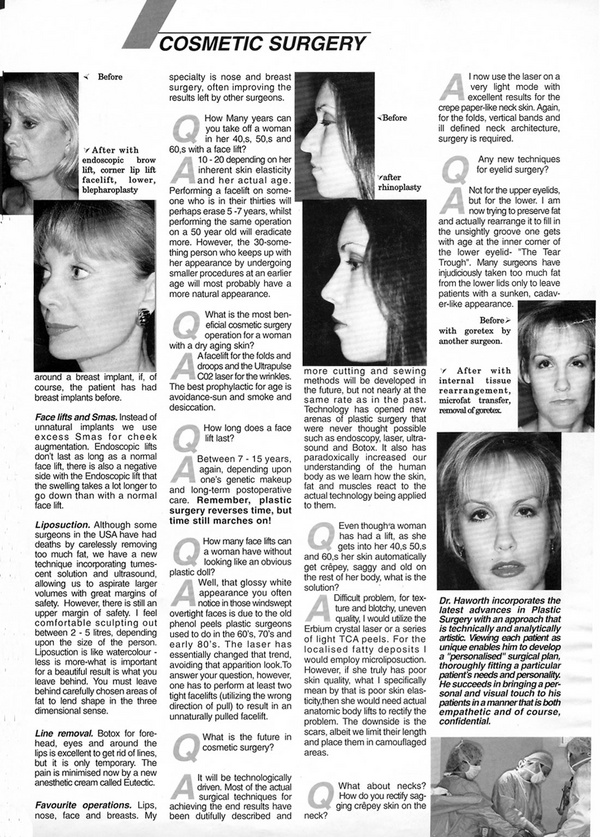
In order to iron our sheets, peels in various fashions or lasers can be applied to render the skin smooth in both maintenance skin hygiene and facials to keep the skin clean and free of toxic buildup. Finally, to actually make the bed, a well performed facelift with fastidious bent towards detail can be utilized in a natural way. The successfully rejuvenated face should attract rather than detract. Unlike cosmetic nasal surgery, performing a facelift (synonyms include rhytidoplasty, meloplasty or rhytidectomy) does not require an innate aesthetic eye. However, it does require a surgeon with a keen eye for details, since it is a surgery of minute details – needed to avoid the tell tale signs of a facelift. This is key to achieving the natural look. Among these tip-off signs are raised, altered hairline, a distorted tragus (the cartilage in front of your ear canal), a “pixie ear” (where the earlobe is attached to the facial skin at the jawline), a widened mouth, obvious scars and tension bands across the face (from pulling too tight and removing too much fat).
What is the difference between a mini lift and a full face lift? A mini facelift deals with jowls and facial laxity only; the neck needs minimal or no treatment and the incisions behind the ear are consequently minimized. A full facelift, on the other hand, addresses both the facial looseness and tackles the aging neck and “turkey gobble.” Wait. The situation gets more complicated. Does your surgeon propose a regular skin lift, a skin lift with SMAS (SubMuscular Aponeurotic System “tightening the facial muscles”), a deep plane lift, a composite lift, a biplanar lift or just an everyday subperiosteal midface lift? It depends on the individual surgeon’s philosophy, which has most probably been influenced by his/her training.
The pendulum is swinging back towards the simpler skin lifts combined with or without some form of SMAS tightening. The more sexy and complicated, deeper facelifts (deep plane and composite) classically produce more swelling with more complications and questionably better results at best.
Long term follow-up studies as judged by independent panels of Plastic Surgeons have failed to demonstrate and difference in outcome and longevity between the techniques.
Where to go from here? Do your homework! There are many Plastic Surgery “practitioners” who masquerade as fully trained Plastic Surgeons eager to offer you their expertise at a great seasonal discount. Ask about their techniques, their “before and afters,” their board certification (The American Board of Plastic Surgery) and the specific training.
Keep in mind, however, that patients must be realistic in their expectation and the surgeon must underscore this. Remember, plastic surgery reverses time but time still marches on.
Dr. Haworth is a Board Certified Plastic Surgeon who practices in Beverly Hills.

In order to iron our sheets, peels in various fashions or lasers can be applied to render the skin smooth in both maintenance skin hygiene and facials to keep the skin clean and free of toxic buildup. Finally, to actually make the bed, a well performed facelift with fastidious bent towards detail can be utilized in a natural way. The successfully rejuvenated face should attract rather than detract. Unlike cosmetic nasal surgery, performing a facelift (synonyms include rhytidoplasty, meloplasty or rhytidectomy) does not require an innate aesthetic eye. However, it does require a surgeon with a keen eye for details, since it is a surgery of minute details – needed to avoid the tell tale signs of a facelift. This is key to achieving the natural look. Among these tip-off signs are raised, altered hairline, a distorted tragus (the cartilage in front of your ear canal), a “pixie ear” (where the earlobe is attached to the facial skin at the jawline), a widened mouth, obvious scars and tension bands across the face (from pulling too tight and removing too much fat).
What is the difference between a mini lift and a full face lift? A mini facelift deals with jowls and facial laxity only; the neck needs minimal or no treatment and the incisions behind the ear are consequently minimized. A full facelift, on the other hand, addresses both the facial looseness and tackles the aging neck and “turkey gobble.” Wait. The situation gets more complicated. Does your surgeon propose a regular skin lift, a skin lift with SMAS (SubMuscular Aponeurotic System “tightening the facial muscles”), a deep plane lift, a composite lift, a biplanar lift or just an everyday subperiosteal midface lift? It depends on the individual surgeon’s philosophy, which has most probably been influenced by his/her training.
The pendulum is swinging back towards the simpler skin lifts combined with or without some form of SMAS tightening. The more sexy and complicated, deeper facelifts (deep plane and composite) classically produce more swelling with more complications and questionably better results at best.
Long term follow-up studies as judged by independent panels of Plastic Surgeons have failed to demonstrate and difference in outcome and longevity between the techniques.
Where to go from here? Do your homework! There are many Plastic Surgery “practitioners” who masquerade as fully trained Plastic Surgeons eager to offer you their expertise at a great seasonal discount. Ask about their techniques, their “before and afters,” their board certification (The American Board of Plastic Surgery) and the specific training.
Keep in mind, however, that patients must be realistic in their expectation and the surgeon must underscore this. Remember, plastic surgery reverses time but time still marches on.
Dr. Haworth is a Board Certified Plastic Surgeon who practices in Beverly Hills.
L.A. TIMES 1996 THE AGE OF DENIAL (1996) – THE AGE OF DENIAL
Memo to All Boomers: How is It That You’ve Transformed the Rite of Turning 50 Into a Celebration of your So-Called Youth?
By
Denis Romero
TIMES STAFF WRITER
So you’re turning 50.
Hahaha. Er, take that back. Maybe the joke’s
on us.
You would think all those yuppie-haters out there would be laughing at the prospect of Dockers-wearing baby boomers going
Grecian, power walking instead of jogging, taking Depends breaks in between puffs of their Arturo Fuentes.
But oh, no. Just the opposite.
Just as in the past, you have managed to turn a
traditional passage of doom into a celebration of your youth and
culture-yet another opportunity to party in the pages of the media that
you so glamorously control. Oldstock?
The Beatles are No. 1 (again
yawn). Everybody wants to sell you a miracle drug. Hollywood
chronicles your every breath (from “The Graduate” to “Forest Gump”). And
one thing’s for sure: As the 76 million of you begin to hit 50 at the
rate of one every 7 1/2 seconds this year, you will change the concept
of aging as much as aging will change you. You are, after all, so vain.
What used to be old will be young-a feat only you
boomers could accomplish. From a new vocabulary (can you imagine
calling Cher a senior?) to age -sensitive marketing (Act Young. Drink
Pepsi!) to new products (girdles for a new generation), the world will
bend over backward to make you feel like lads and lassies (though you
will go through more life changes than an Oliver Stone plot).
“Fifty is still an age where you can still have one
foot in youth,” insists 43 they’ve even invented a new name for middle
aged . They call it “mid-youth,” Mister. “No one here talks about
middle aged people,” says Alison Kaar, spokeswoman for Lens Crafters.
“We call them emerging presbyopes.” “Presbyopes” refers to the
farsighted, as far as we can see.
“The story in
marketing is not selling to how old people are,” Kamins says, “but the
age people think they are.”
And boomers
measure themselves as much as 15 years younger than their chronological
age, experts say. Or as Gail Sheehy put it in “The New Passages,”
(Random House, 1995) her paean to incessant self-improvement, “Fifty is
now what 40 used to be.” Mercedes-Benz is hip to that. In a twist of
advertising irony, the German car company is invoking a famous line from
’60s singer Janis Joplin: “Oh Lord, won’t you buy me a Mercedes-Benz.”
Redkin hair, skin and body products have a new motto: “To Preserve and
Protect.” And Revlon is using a beautiful Melanie Griffith, 37, to
promote “Age Defying Makeup.”
Then
there’s the Circuit City commercial that portrays a suited yuppie
out-blasting a grunge rocker in a park-bench boom box battle. (As if.)
Or the Caffeine Free Diet Coke commercial that has an older woman
boxing a younger man and winning. A Coca-Cola marketing spokesman is
proud to say, “It’s the first ad campaign in the soft-drink industry
dedicated to the 40-plus market. No caffeine. No sugar. No limits.”
Will you ever age? “What we can look forward to
is people who not too long ago were staring at lava lamps, smoking dope
and listening to Iron Butterfly – they’re basically going to be in
diapers,” says Bob Garfield, editor at large for Advertising Age
magazine. “How are advertisers going to reach those people? I don’t
think its going to be pretty. I can actually envision Jimi Hendrix
being invoked to sell Arthritis Pain Formula. It’s going to be a laugh
riot.”
Even girdle and butt-pads, the
untouchable domain of grannies, are being marketed as Slenderizing
Manshape Undergarments, Super Shaper Briefs and Bottoms Up Corsets.
(If these don’t work, sagging body parts will no doubt be the next
big thing. You’ll call it skin relaxation-and twentysomthings will be
stretching their chins and cheeks just so they can fit in.)
Plastic surgery is at an all-time
high among boomer men, according to the American Society of Plastic and
Reconstructive surgeons. Dr. Randal Haworth, a
Beverly Hills plastic surgeon, estimates that one out of four of his
patients is male–and most of those are boomers. “What’s so ironic,”
says the 34 year old, is that these are the same people who espoused
protest and 30 years later are succumbing to modern pressure, the
antithesis of what the ’60s stood for.”
Punk.
But
he’s right. Pectoral and penile implants are in. Breasts are back.
And everybody wants a nip-and-tuck (though they don’t call them face
lifts anymore, of course: “facial rejuvenation” is the proper term).
THE NEW YORK TIMES (1996) – AS INSURERS CUT FEES, DOCTORS SHIFT TO ELECTIVE PROCEDURES
By MILT FREUDENHEIM
Published:
August 24, 1996
Dr. Phillip Haeck, a Seattle plastic surgeon,
used to spend half his working hours rebuilding the breasts of cancer
patients and performing other reconstructive procedures. Then
managed-care companies started to cut his fees by 60 percent or more.
So
Dr. Haeck switched to cosmetic procedures that insurers do not cover,
like breast enlargement. No longer restricted to the $1,980 fee that
insurers allowed him for a six- to eight-hour breast restoration, he can
now earn $3,800 for inserting saline breast implants, which takes two
hours or less.
He was surprised by how many women were willing to
pay. His income has already recovered, he said, and his working day now
ends an hour earlier because he deals with far fewer insurance forms.
Just
as Dr. Haeck has done, thousands of doctors, frustrated by the price
controls, red tape and sometimes intrusive oversight of managed care,
have begun building lucrative practices in fields like cosmetic surgery,
correcting myopia with lasers, and infertility treatment, where
patients will pay even when insurers will not.
Insurance
companies refuse to pay for many of these elective procedures, arguing
that they are not medically necessary or are still experimental. But a
growing number of Americans are willing to spring for them — at
handsome prices. Indeed, while it used to be assumed that a doctor could
charge a higher fee when an insurer was helping to foot the bill, the
opposite is now true in many cases. Fees are often far higher than those
doctors can charge under managed care for work requiring comparable
skill and time.
The doctors increasing their emphasis on such
procedures include:
*Physicians doing more cosmetic surgery,
including plastic surgeons, dermatologists, ophthalmologists, ear, nose
and throat specialists, dentists, gynecologists and general
practitioners. Among the most common procedures are breast enlargement;
removal of wrinkles, furrows and bags under the eyes; face lifts; nose
jobs; hair transplants for men; vein surgery; chemical peels of
unsightly skin, and liposuction to remove fatty tissue. The fee for such
procedures can range from a few hundred dollars to more than $20,000.
*Ophthalmologists,
who typically receive less than half the $2,000 that they used to get
for each lens implant for cataract patients, shifting to a new surgery
that uses lasers to correct nearsightedness — and charging $1,500 to
$2,000 an eye.
*Some ear, nose and throat specialists — whose
fees have been cut 40 percent to 60 percent under managed care — now
capitalizing on a new technique: using lasers to eliminate snoring by
removing tissue from the uvula at the back of the tongue. A typical fee
is $2,500.
*Some obstetrician-gynecologists with special training
in infertility services now averaging $2,000 and more for in vitro
fertilizations.
*Some urologists, whose surgical fees have
dropped to $600 from $1,400 for treating enlarged prostate glands, now
making a business of penis-enlargement surgery. Those fees range from
$4,800 to $7,000.
To be sure, the overwhelming majority of the
nation’s 650,000 physicians are still deeply enmeshed in managed care
and are not reaching out for more lucrative niches like these. But there
is wide agreement in the medical community that as the number of
procedures that do not qualify for insurance coverage — and the
popularity of such procedures — grow, a rising number of doctors are
making the most of this.
One reason that these specialists can
find enough takers paying out of their own pockets is the stunning
increase in family income of the wealthiest Americans. The average
income for the top 20 percent of households grew to $105,945 in 1994
from $73,754 in 1968, a jump of 44 percent after adjusting for
inflation, according to the Census Bureau. That has occurred even as the
number of uninsured people grows and as many people see their own
medical benefits reduced.
Also, some doctors and patients have
found imaginative ways to get insurers to pay part of the bill. Nose
jobs can get some insurance coverage if the doctor indicates that the
patient has had trouble breathing. Some dermatologists who remove spider
veins can get insurers to pay by calling them artery-blocking varicose
veins.
The physicians’ rush to such procedures is not surprising.
Managed care has been cutting the flow of patients and sharply reducing
fees for many specialists, notably dermatologists, ophthalmologists,
ear, nose and throat specialists, general surgeons, cardiac and vascular
surgeons, cardiologists, anesthesiologists and gastroenterologists,
said Dr. Richard Doyle, a management consultant in St. Louis with the
Milliman & Robertson consulting firm.
No one tracks the
number of doctors performing procedures not covered by insurance or how
that number has changed, but there are many indications that it is
growing. For example, the number of board-certified plastic surgeons
rose 75 percent, to 5,200 in 1994, from 2,980 in 1980, according to the
latest available surveys by the American Medical Association. And last
year 40 percent of plastic surgeons said cosmetic work was now their
main business, up from 32 percent in 1991, according to the American
Society of Plastic and Reconstructive Surgeons.
The American
Academy of Cosmetic Surgery said the number of commonly performed
cosmetic procedures doubled, to 1.09 million, between 1990 and 1994, the
latest available year.
Dr. Randal Haworth, a
Beverly Hills, Calif., plastic surgeon, said that by concentrating on
cosmetic surgery, ”We are not held fiscal and emotional hostage by
these people in managed care; secondly, by refusing to join their plan,
you are not obligated to accept what they pay.”
Dr. Haeck, the
Seattle plastic surgeon, said he shifted to 90 percent cosmetic surgery
from a practice that was half cosmetic and half reconstructive, after
price-cutting insurers threatened to reduce his income by 30 percent.
For instance, he said, his share of fees for breast reconstruction after
cancer surgery dropped to $1,980 from $3,800.
Dr. Haeck resigned
from eight managed-care networks, freeing more time for
breast-enlargement procedures that he said bring in around $3,800 each.
He
hired a marketing expert to, as he put it, ”ramp up that side of the
business.” Dr. Haeck also began giving seminars at a local athletic
club and appearing on local television, and he changed his
advertisements to feature his cosmetic services.
Dr. Gwendolyn
Maxwell Davis, a cosmetic surgeon in Tucson, Ariz., took one look at the
field of plastic surgery when she finished her training and decided to
devote herself exclusively to cosmetic procedures. She charges $6,000
for a face lift, $4,500 for breast enlargement, and $4,500 for a ”tummy
tuck.” All told, she expects to net $450,000 this year, after only two
years in practice.
Another fast-growing niche is infertility
treatment. The American Society for Reproductive Medicine reported
32,000 cycles of in vitro fertilization were initiated in 1993, the most
recent year for which numbers were available, up 76 percent from 1989.
And physicians say that the number has grown significantly since then.
”From
a purely financial point of view, I’d rather not have managed care
involved,” said Dr. Ira Charlip, a San Francisco urologist who
specializes in infertility. ”I can charge the patient a reasonable
amount and they pay 100 percent of it.”
Advances in laser
technology have opened numerous new medical opportunities as well, many
not covered by insurance. Some are cosmetic, like burning off tattoos
and age spots, zapping wrinkles and removing hair.
Other
procedures, which some insurers cover, include removal of disfiguring
birthmarks. New laser procedures are growing much faster than older
procedures covered by managed care, Irving Arons, managing director of
Spectrum Consulting in Peabody, Mass., said.
”Doctors are
looking for new ways of generating revenue,” said Larry Haimovitch, a
medical technology consultant in San Francisco. ”If they can buy a
laser machine and pay it back quickly, they do it.”
Some of the
newest lasers are used to treat myopia by changing the shape of the
eyeball. Dr. Frank O’Donnell, a St. Louis ophthalmologist, had
encountered big reductions in what insurers allowed for cataract
surgery. ”It’s pretty hard to scramble to replace a 50 percent
reduction in reimbursement,” he said.
Now, Dr. O’Donnell
specializes in laser treatments for myopia at $1,500 to $2,000 an eye.
He is also chairman of Lasersight Inc., a start-up company that he said
was testing a second-generation laser for myopia.
Dr. O’Donnell
laments the changes in the medical business brought on by managed care,
and says he worries about whether the most talented doctors will flee to
other professions.
”Ophthalmology has gone from being an
exciting, very valued specialty to something that is not very desirable
anymore,” he said. ”It’s painful — we used to be able to attract some
of the very best doctors.”
Mr. Arons of Spectrum Consulting
said that there were at least 50 laser vision centers in the country,
each with several physicians. He projects 200 centers by the end of the
year and a million procedures a year by 2000 at $1,000 each as the price
of the equipment comes down — a $1 billion market.
Dr. Roy
Geronemus, director of the Laser and Skin Center of New York, which does
both insured and uninsured procedures, said attendance had increased
sharply for his course in new laser techniques at New York University
Medical Center. Some of his students, he said, are physicians ”who are
looking for ways to circumvent the constraints on medical
practice.”