
|
As a primary and revision rhinoplasty specialist, Dr. Randal Haworth of Beverly Hills excels with all types of complicated nose jobs, but sometimes it is a simple pleasure to be confronted with a classic reduction rhinoplasty. Though these are relatively simple in concept, all nosejobs (or rhinoplasties) must be handled with utmost care and dedication to excellence.
Why does a prospective patient consult with me requesting a nosejob?
Well, most come to me with the latter concerns such as: “Doc, my nose is just too big for my face”, “I always hated my hump”, “My tip is falling like a bird’s beak”, etc., etc. Upon examination, the nose will usually manifest the aforementioned undesirable characteristics to varying degrees:
Check out this patient, who underwent a classic reduction rhinoplasty on the Swan. Here is a typical example of a classic reduction rhinoplasty,even though only subtle changes were performed. Note that a radix graft (to raise the nasal frontal angle) was placed to add height and therefore elegance to her nose. For a more general overview of rhinoplasty, go to: http://www.drhaworth.com/rhinoplasty/ |
||||||||
|
Tag: Beverly hills rhinoplasty specialist


The Radix Graft in Rhinoplasty
|
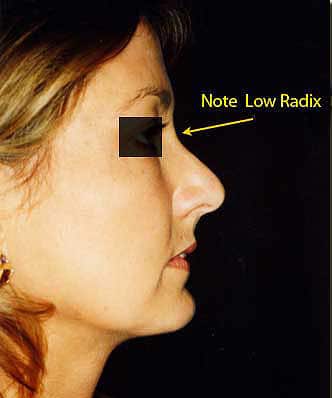
This lesser known anatomic point of the nose is often purposely overlooked by rhinoplasty specialist surgeons because of the challenges it poses to those attempting to alter it. It is represented by the angle formed by the uppermost portion of the nose as it blends into the forehead proper. Yes, altering this area does have a subtle, yet profound influence upon the final appearance of a nose job- it can differentiate an excellent result from a “so-so” one. The surgeon can raise the radix so that the nose blends into the forehead at a higher latitude as well as softly elevate the natural valley that can exist at this are if it is too deep. Furthermore, one can deepen the radix if too much bone is present between the eyeball and the bridge on profile view.
The ideal position of the radix lies approximately at the latitude of the upper eyelash/upper eyelid crease. Beverly Hills plastic surgeon, Dr Randal Haworth can raise it by placing a precisely shaped softened cartilage graft (usually harvested from the nasal septum or ear) with beveled edges onto the bone of the radix area. Alternatively the radix or nasion can be rasped or chiseled with specialized delicate instruments to a lower, deeper position. Why does raising a radix from a low position improve the final appearance of a nose? Well, imagine two noses which are identical in shape and forward projection except that one has a low radix while the other has a high one. The one with the low radix is shorter compared to the one with the high. Now imagine two men, both with the same 34 inch waist, but one is short while the other tall. Who appears fatter? The short person does, of course. This same optical illusion applies to the nose with a low radix-it appears as it projects further out from the face as compared with the one with the higher radix and not necessarily in an attractive way. The following photos represent a beautiful result of a corner lip lift and concomitant rhinoplasty in which the radix was raised. |
|||||||
|
|||||||
| Work here results in some extra swelling localized to the space between the eyebrows in the sense that it lasts a few days longer. Dr Haworth at the Haworth Institute has a few tricks up his sleeve to accelerate the resolution of the nasal swelling by injecting a dilute mix of Kenalog under the skin (and it is relatively painless) two weeks out. This “turbocharges” the swelling to go away! Of course, the radix can also be augmented with a filler of some sort, such as fat, Radiesse, Juvederm, Aquamid and Artefill. | |||||||

The Injectable Nosejob
In the era of Twitter, Facebook, texting, rapid- fire music video editing, etc. everyone (including those not diagnosed with ADD) wants instant results. So what is unusual with wanting an instant nose job or rhinoplasty? Absolutely nothing. An instant nosejob is performed by strategically injecting a pre-chosen filler just below the nasal skin in an aesthetically sensitive manner. Temporary fillers such as Hyaluronic acids (Restylane™, Perlane™, Juvederm™, etc.) and calcium hydroxyappatite (Radiesse™) may be used as a “dress rehearsal” to confirm if the patients like their result. If so, many will then opt for a more permanent filler, either in the form of fat, Artefil ™ or Aquamid ™ (which is not yet FDA approved).
The appeal is obvious: less bruising, less prolonged swelling, less initial expense, less scary for the wary and more predictable (in the proper hands) with less risks. However, the injectable technique cannot be used to correct all types of cosmetic nasal problems and deformities. This is especially true for noses that need to be reduced in size and refined in shape. One does not need to be a genius to realize that fillers may do little to make a nose smaller by removing humps, refining tips and narrowing bones, no matter how well injected they are. The ideal candidate for an injectable rhinoplasty is the nose that needs to be augmented, either via it’s bridge (or dorsum) or it’s tip or both. A drooping tip can be elevated only to a subtle degree with filler.
Filler is also a great solution to those noses that have minor irregularities stemming from prior rhinoplasties. Filler will generally not help breathing problems. To learn more about this elegant solution to a rather common problem, check out these videos:
1.Extra Injectable NoseJob
2.Today Show Injectable NoseJob
3.Extra Artefill Injectable revision rhinoplasty
Dr Randal Haworth of Beverly Hills counts primary and revision rhinoplasty as one of his specialties of plastic surgery
The appeal is obvious: less bruising, less prolonged swelling, less initial expense, less scary for the wary and more predictable (in the proper hands) with less risks. However, the injectable technique cannot be used to correct all types of cosmetic nasal problems and deformities. This is especially true for noses that need to be reduced in size and refined in shape. One does not need to be a genius to realize that fillers may do little to make a nose smaller by removing humps, refining tips and narrowing bones, no matter how well injected they are. The ideal candidate for an injectable rhinoplasty is the nose that needs to be augmented, either via it’s bridge (or dorsum) or it’s tip or both. A drooping tip can be elevated only to a subtle degree with filler.
Filler is also a great solution to those noses that have minor irregularities stemming from prior rhinoplasties. Filler will generally not help breathing problems. To learn more about this elegant solution to a rather common problem, check out these videos:
1.Extra Injectable NoseJob
2.Today Show Injectable NoseJob
3.Extra Artefill Injectable revision rhinoplasty
Dr Randal Haworth of Beverly Hills counts primary and revision rhinoplasty as one of his specialties of plastic surgery
The pinched nose; the rhinoplasty gone “wrong”
Everyone undergoing elective cosmetic surgery truly expects their results to be exemplary and rarely contemplate what they will do if something does not turn out as they expected. Rhinoplasty, or nose job surgery, is one of the most challenging sub specialties in aesthetic plastic surgery and Dr Randal Haworth is one of the leading specialists in revision rhinoplasty. Despite the fact that the nasal area is generally less than 2″ x 1″ x 1 ” in dimension, a small amount of unpredictability always exists in terms of obtaining the “perfect result”. Of course, the more experienced and better the nasal surgeon is, the more he or she is able to harness that unpredictability and secure an excellent result.
Among the more common complications that occur from a rhinoplasty are asymmetry, difficulty breathing, incompetent internal nasal valves (inverted V deformity) and a pinched tip. Modern rhinoplasty techniques involve far more subtle maneuvers than old-fashioned cutting out cartilage and breaking bones. Since the shape of the nasal tip is determined both by skin thickness and the underlying shape of the nasal cartilages, it used to be taught that to avoid a pinched nasal tip, all the surgeon has to do is avoid cutting out too much cartilage. Otherwise, the nostrils will loose the supportive function of the cartridges and collapse upon themselves thus leading to a “pinch tip” appearance. In actuality, the situation is more complicated than that. While it is indeed important to leave enough catilage as support, modern techniques of rhinoplasty involve delicately placing precise sutures in order to control the tip and projection of the nasal tip. If the knots are tied ever so slightly tighter than normal, the supportive nature of the cartilage may be overcome by the scar tissue that will develop in the postoperative period. The cartilages will then become concave in appearance thus leading to a pinched tip as seen in the accompanying photo.

Preoperative nasal deformity after previous rhinoplasty. Note inverted “V” deformity, asymmetry and pinched tip
Also seen in this photo is an inverted “V” deformity. This occurs when the upper lateral cartridges separate away from the midline septum as well as the upper nasal bones. This results in an irregularly appearing nose along its bridge on full frontal view including an altered brow-tip curvilinear line.
Both a pinch tip and an inverted “V” deformity can result in difficulty breathing through the nose. Correction as part of a revision rhinoplasty involves carefully separating the cartilage from the surrounding scar (which may appear deceptively similar in texture and look during surgery) and carefully placing precisely defined cartilage grafts on to the pre-existing weakened cartilage as support. Spreader grafts are needed to correct an inverted “V” deformity. These are small strips of cartilage fashioned from either the septum or ear which are secured between the midline septum and the inner border of the upper lateral cartilage is-in effect, reconstructing the middle vault up the nose. If this remains uncorrected, not only does the visual deformity processed, but nasal obstruction will also occur upon inspiration. This occurs in a similar fashion to a loose canvas roof of a tent which gets sucked in by high mountain winds.
The postoperative photo of the same patient clearly demonstrates the correction of the pinched tip and inverted “V” deformity via cartilage placement, scar removal and judicious fracture of the nasal bones. I also be rotated the tip in order to make the nose look “less done”.
To cut a long story short, added support in the form of cartilage is needed to correct the weakness in the form and function resulting from a rhinoplasty gone awry. Rhinoplasty is similar to a chess game. It is the only surgery that takes me longer to perform than I did 10 years ago. This is because I recognize and deal with any potential pitfalls that may result during the initial surgery. I have to think several steps ahead similar to a game of chess. Finally, not only do I have to make the nose look beautiful, but I have to erase all evidence that anything had been performed by a human hand. this takes time, aesthetic sensibility and patience.
This video shows how a pinched tip can be successfully repaired:
For further information about what one may expect after a rhinoplasty click here
For further information go to www.drhaworth.com or call his office in Beverly Hills to schedule a consultation.
Among the more common complications that occur from a rhinoplasty are asymmetry, difficulty breathing, incompetent internal nasal valves (inverted V deformity) and a pinched tip. Modern rhinoplasty techniques involve far more subtle maneuvers than old-fashioned cutting out cartilage and breaking bones. Since the shape of the nasal tip is determined both by skin thickness and the underlying shape of the nasal cartilages, it used to be taught that to avoid a pinched nasal tip, all the surgeon has to do is avoid cutting out too much cartilage. Otherwise, the nostrils will loose the supportive function of the cartridges and collapse upon themselves thus leading to a “pinch tip” appearance. In actuality, the situation is more complicated than that. While it is indeed important to leave enough catilage as support, modern techniques of rhinoplasty involve delicately placing precise sutures in order to control the tip and projection of the nasal tip. If the knots are tied ever so slightly tighter than normal, the supportive nature of the cartilage may be overcome by the scar tissue that will develop in the postoperative period. The cartilages will then become concave in appearance thus leading to a pinched tip as seen in the accompanying photo.

Diagram showing severe nasal deformity after a previous nosejob

Preoperative nasal deformity after previous rhinoplasty. Note inverted “V” deformity, asymmetry and pinched tip
Also seen in this photo is an inverted “V” deformity. This occurs when the upper lateral cartridges separate away from the midline septum as well as the upper nasal bones. This results in an irregularly appearing nose along its bridge on full frontal view including an altered brow-tip curvilinear line.
Both a pinch tip and an inverted “V” deformity can result in difficulty breathing through the nose. Correction as part of a revision rhinoplasty involves carefully separating the cartilage from the surrounding scar (which may appear deceptively similar in texture and look during surgery) and carefully placing precisely defined cartilage grafts on to the pre-existing weakened cartilage as support. Spreader grafts are needed to correct an inverted “V” deformity. These are small strips of cartilage fashioned from either the septum or ear which are secured between the midline septum and the inner border of the upper lateral cartilage is-in effect, reconstructing the middle vault up the nose. If this remains uncorrected, not only does the visual deformity processed, but nasal obstruction will also occur upon inspiration. This occurs in a similar fashion to a loose canvas roof of a tent which gets sucked in by high mountain winds.
The postoperative photo of the same patient clearly demonstrates the correction of the pinched tip and inverted “V” deformity via cartilage placement, scar removal and judicious fracture of the nasal bones. I also be rotated the tip in order to make the nose look “less done”.

After revision rhinoplasty by Dr Haworth, including placement of spreader and lateral crural strut grafts
This video shows how a pinched tip can be successfully repaired:
For further information about what one may expect after a rhinoplasty click here
For further information go to www.drhaworth.com or call his office in Beverly Hills to schedule a consultation.
The Tricky Rhinoplasty and Upper Lip Lift Combination Surgery
While many surgeons feel uncomfortable with performing an upper lip lift, let alone one simultaneously with a rhinoplasty, it can be safely done. The concern revolves around the fear of losing vital blood supply to the columella (the fleshy straight partition that exists between the nostrils), because if the blood flow is compromised to this area then necrosis or loss of the columellar skin can result. This, in turn, can lead to a possible unsightly scar. If the nose job is performed through an endonasal or closed approach ( whereby all incisions are strictly confined to within the nose itself) there should be little concern for this. However, caution must be exerted when the rhinoplasty is performed with an open technique- one that involves making a scar across the columella in order to gain better access and therefore better visualization and control of the operation. In a normal open technique the incision is placed about halfway up on the columella. Since an upper lip lift necessitates making an incision at the base of the columella (where it joins with the upper lip), the incision needed for the open rhinoplasty can also be the same one- so the incision will be used for two different purposes.
The situation becomes more complicated, however, when a persisting scar stemming from a previous open nose job is present. In this situation, the plastic surgeon must carefully plan his incisions so as not to compromise the blood supply. More often than not it is safer to keep the upper lip lift incision separate from the rhinoplasty’s in these revision cases.
The planning becomes even more critical when the nostrils need to be narrowed during the nasal aesthetic surgery ( Weir excisions). Not only does the upper lip lift need to be blended well onto the columella, but it also needs to be conformed to a freshly narrowed nasal base, with minimal undesired tension across the final scar ( which can increase the chance of it being noticeable). Intricate surgery along with an intimate knowledge of the regional anatomy and the biophysics of an upper lip lift are key ingredients to a beautiful outcome in this combination surgery. Following are two examples of before and afters of this combo surgery.
To view more upper lift results go to:http://www.drhaworth.com/procedures/upper-lower-lip-lifts/

Scar placement for rhinoplasty alone and in combination with an upper lip lift
To view more upper lift results go to:http://www.drhaworth.com/procedures/upper-lower-lip-lifts/

Patient 1.Preop: 52 year old female

After Rhinoplasty with Weir excisions, Upper lip and corner Lip Lifts along with a lower V-Y plasty
Note the improved visual interplay between the nose and upper lip along with youthful tooth show and narrower oral span.

Patient 2.Preop: 35 year old. Note lack of upper tooth show and nasal tip disharmony
 Postop after Rhinoplasty, upper lip lift, lower V-Y platy and lip fat transfer
Postop after Rhinoplasty, upper lip lift, lower V-Y platy and lip fat transfer
Rhinoplasty Philosophy – Dr. Randal Haworth
Rhinoplasty, or what people refer to in colloquial parlance as “nose job” surgery, is one of my favorite specialities. I have performed literally thousands of these challenging procedures as far afield as the Middle East, Europe and South East Asia. What I find so fascinating about rhinoplasty is how it can impart such dramatically positive change to the face as a whole – a classic case of the final result being greater than the sum of it’s parts.
Not only do I find it immensely gratifying to invent new solutions to challenging problems, I actually like the ” feel” of the surgery- the intricate interplay between skin, cartilage and bone. Even after 16 years of private practice, I discover new, exciting nuances in techniques that the average surgeon performs without feeling. Though I considered myself “top of my game” at the time I was doing plastic surgery on ” The Swan” in 2004, I look back upon those patients today and realize I could do better on a third of those rhinoplasties I performed! Like an artist, I always aim to do better and realize that my work today is better than it was in 2004 and will be better still 5 years from now, barring some personal tragedy.
The first era for me in rhinoplasty surgery was about creating beauty and my second era is about controlling beauty- imbuing a subtle softness into the result, and erasing all signs that humans hands had anything to do with the patient”s nose. A good pianists doesn’t just play the notes and chords accurately but also with crescendo and pianissimo- with feeling. My next series of blog posts will revolve around the subject of nasal surgery and aim to share with you certain concepts, both basic and advanced, that are important to both the lay person and surgeon alike.
Dr Randal Haworth of Beverly Hills is a specialist in all forms of aesthetic plastic surgery including primary and revision rhinoplasty.For further information go to drhaworth.com
Not only do I find it immensely gratifying to invent new solutions to challenging problems, I actually like the ” feel” of the surgery- the intricate interplay between skin, cartilage and bone. Even after 16 years of private practice, I discover new, exciting nuances in techniques that the average surgeon performs without feeling. Though I considered myself “top of my game” at the time I was doing plastic surgery on ” The Swan” in 2004, I look back upon those patients today and realize I could do better on a third of those rhinoplasties I performed! Like an artist, I always aim to do better and realize that my work today is better than it was in 2004 and will be better still 5 years from now, barring some personal tragedy.
The first era for me in rhinoplasty surgery was about creating beauty and my second era is about controlling beauty- imbuing a subtle softness into the result, and erasing all signs that humans hands had anything to do with the patient”s nose. A good pianists doesn’t just play the notes and chords accurately but also with crescendo and pianissimo- with feeling. My next series of blog posts will revolve around the subject of nasal surgery and aim to share with you certain concepts, both basic and advanced, that are important to both the lay person and surgeon alike.
Dr Randal Haworth of Beverly Hills is a specialist in all forms of aesthetic plastic surgery including primary and revision rhinoplasty.For further information go to drhaworth.com